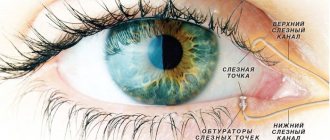
Signs and causes of dry eyes when wearing contact lenses
There are several symptoms that indicate increased dryness of the mucous membranes of the organs of vision. For those who constantly use lenses, dry eye syndrome is manifested by the following symptoms:
- Constant sensation of the presence of a foreign object.
- Increased fatigue - it becomes impossible to look at an object for a long time, work, or read.
- Redness of the membranes.
- Problems with clear images.
- Feeling of sand in the eyes.
All this becomes the reason for refusing to wear optics of this kind.
There is a whole list of reasons against which the syndrome develops. Among them:
- Failure to comply with the wearing regime and timely replacement of the product: if a person wears them longer than according to the instructions, leaves daytime ones at night, and also does not change them on time, then problems are possible.
- Using care products that are not suitable for lenses: Many people try to use multi-purpose solutions to instantly solve a complex of problems, but they do not include softening components and do not moisturize the lenses. The latter dry out faster and cause dryness.
- Incorrect fitting (fitting) of optics: contact lenses that do not fit correctly on the cornea do not allow tear fluid to circulate normally.
Failure to follow simple hygiene rules can lead to unpleasant consequences. Therefore, you need to carefully monitor your health and worry about the condition of your contact devices in a timely manner. Rules for wearing contact lenses are described here.
Help with dry eyes
Prevention and treatment of dry eyes is carried out using various moisturizers and folk methods.
Artificial tear preparations
They are used to additionally moisturize the cornea of the eye when there is a deficiency of tear fluid. Drops create a protective film on the surface of the eye and prevent tear evaporation. They are good for relieving symptoms of dryness, but can irritate the eyes if used frequently.
Artificial tear preparations vary in consistency. Thinner ones last less time than thick ones.
Before using the drops, the lenses are removed for 15 minutes and applied every few hours.
Eye ointments
Eye ointments have a more viscous consistency than drops. In doing so, they not only eliminate the symptoms, but also help cure the problem of dry eyes. Before using them, you need to remove your contact lenses for 15-20 minutes . They have greater effect when used at night. However, eye ointments are not recommended to be used together with drops.
Treatment
If dryness appears while wearing optics of this kind, treatment should begin. Special drops are added to lubricate the cornea. It could be Cornergel. This is a drug based on dexpanthenol, which has regenerating properties. This product is in the form of a gel. It is viscous, which helps the drug stay on the mucous membrane longer. 1 drop of gel is instilled into the lower part of the conjunctival sac 4 times a day. Additionally, you need to apply one drop before bed. After instillation, gently massage the eye so that the medicine is distributed evenly. The best moisturizing drops for wearing lenses are reviewed here.
In a situation where drugs do not help, surgery is prescribed - doctors will close the tear ducts so that the fluid accumulates and does not leave quickly.
It is also necessary to study the condition of the optics - doctors suggest replacing the care product so that the mucous membrane calmly perceives a foreign object.
Take care of prevention:
- Compliance with the wearing and replacement regimen, the use of high-quality solutions, etc.
- Use sunglasses if necessary - this way ultraviolet radiation will not further irritate and injure your eyes.
- Ensure sufficient humidification of the air in the room, especially when it is hot from radiators; in the summer, the eyes suffer from air conditioning.
- When working at a computer monitor, give your eyes plenty of rest. The same applies to reading books and other variants of the target load, when maximum visual concentration is required. You need to give yourself the opportunity to blink thoroughly so that the mucous membrane is evenly moistened with liquid.
- Place the screen of your device – phone, computer, e-reader – at a short distance below eye level. They will not open wide; a smaller volume of liquid will evaporate from the surface of the apple.
- It is regularly necessary to use preparations such as artificial tears - they moisturize the mucous membrane and provide comfort. Consult your doctor about the product you choose.
- Give up such a bad habit as smoking - cigarette smoke irritates the mucous membrane and leads to dryness of the mucous membrane.
What to do if your cornea is dry
Treatment of dry eyes involves the following measures:
- compensation for lack of tear fluid;
- elimination of pathologies of the cornea and conjunctiva;
- relief of systemic diseases that can cause hypofunction of the lacrimal glands.
To restore the tear film, hydrophilic gels, emulsions and drops are used. The preparations differ in density, active ingredients and type of preservatives. The composition of therapeutic agents may include artificial polymers, hyaluronic acid, lipids, etc.
The list of effective drops for dry eyes when wearing lenses includes:
- Optimed;
- Maxima Revital Drops;
- ReNu;
- OptiFree;
- Systane;
- Comfort Drops.
You can relieve fatigue and reduce dryness when working at a computer with the help of eye exercises.
Drops for dry eyes
Complications
By ignoring unpleasant symptoms or continuing to fail to comply with simple hygiene and prevention requirements, you risk serious complications. These include a whole list of problems.
Feeling of speck, sand
Normally, the front surface of the eye has a three-layer coating of tear film. Tears are not just a manifestation of emotions, they are also a liquid that performs a number of important functions:
- smoothing of existing irregularities on the cornea;
- hydration;
- ensuring normal breathing and nutrition of eye tissue.
The tear is distributed evenly over the surface of the eye at the moment of blinking. If there is not enough tear fluid or the film is broken, the cornea and conjunctiva dry out. Against this background, a deficiency of oxygen and various nutrients appears. Against this background, the feeling of a speck or sand appears. You can learn about drops for dry and tired eyes here.
Eyes get tired quickly
The number of blinks during painstaking work decreases, the eye is not moisturized, and tear fluid does not wash away dust and various deposits from the surface of the cornea. Against this background, the eyes begin to get very tired. You can use the drops for computer eye fatigue discussed in this material. This is manifested by the following symptoms:
- Redness of the mucous membrane can vary: from mild to severe.
- The appearance of a burning sensation and increased tearfulness.
- Painful sensations.
What to do if it does not stick to the eye
Even people who are experienced in using contact lenses face this problem. The person puts the item on the wrong side. It may not stick due to a manufacturing defect - you need to go to the store where you bought the lenses and demand a return. Problems also arise when the rules for operating optics are violated.
Crumpled or torn
This happens due to several reasons:
- Optics are not of the best quality: uncertified products at a low price do not guarantee ease of use.
- Incorrect use of the product.
- Drying of an object directly in the eye.
- Spicy manicure.
- Expiration date.
Before putting it on, you need to examine the product externally, inspect it in the light, and evaluate its integrity. If there is even the slightest sign of a micro-fracture, you should not use such options.
My vision becomes cloudy
Cloudiness usually appears in a complex. So, it can develop against the background of a chronic infection of the mucous membrane. The problem also develops with intolerance to lenses and against the background of drying out of the mucous membrane. In this case, the picture may appear fuzzy, blurry and dim.
What to do if it’s stuck to the eye, gets in the way and can’t be removed
This usually appears during the adaptation period, when a person is just getting used to the lenses, due to excessive dryness, due to the incorrect position of the object on the mucous membrane, when putting them on with wet hands and untimely removal.
Carefully locate the lens and gently move it. It is necessary to moisturize the eye so that it does not get stuck. If you can't solve the problem on your own, ask for help.
If you feel pain and discomfort when wearing
Cutting, like many other complications, develops against the background of drying out of the cornea and improper use of the optics. You need to remove the lenses, restore eye health, and then try again, using all the recommendations of specialists.
Prevention of constant drying of the cornea
- When concentrating on a computer or smartphone screen for a long time, the eye rarely blinks and the cornea dries out faster. Therefore, it is necessary to take regular breaks to give your eyes a rest and blink as usual.
- Five-minute eye gymnastics improves blood supply to the eye structures, prevents the progression of myopia or farsightedness, improving refraction. There are many gymnastics machines and exercises online that are easy to remember and practice regularly.
- Dusty rooms and places with low humidity should be avoided; in dusty weather it is advisable to wear glasses. In summer, do not forget about sunglasses, as your eyes need additional protection.
Reference. Cigarette smoke causes dry corneas, so you should avoid being around people who smoke.
From the video below you can learn how to perform exercises that will help relieve dry and tired eyes:
Papillary conjunctivitis
It is an inflammation of the mucous membrane caused not by infection. Against the background of this pathology, papillae begin to grow in the eye. This pathology occurs in 15% of cases.
The larger the papillae become and grow, the following will appear:
- burning and itching;
- redness of the mucous membrane;
- increased amount of mucous discharge;
- increased photosensitivity;
- problems with vision clarity and others.
The disease is treated with medications as prescribed by a doctor. Usually a comprehensive option is offered:
- Rinse with Furacillin (1 tablet in a glass of warm water and wipe the eyes with a cotton pad 3-4 times a day);
- Using antiallergic drops, for example, Cromohexal (1-2 drops in each eye according to the instructions);
- To relieve inflammation, Visin drops (a couple of drops in each eye);
- Solcoseryl gel - put under the eyelids on a cotton swab.
The main thing is to follow the course suggested by the doctor. The duration of the course is determined by the severity of the situation.
Wearing soft contact lenses and dry eye syndrome
Description
Soft contact lenses (SCLs) have now not only become widely accepted in ophthalmic practice, but have even penetrated beyond it into the field of cosmetology.
The widespread use of SCLs for the correction of refractive errors, for therapeutic and cosmetic purposes, has made it possible to identify a number of serious problems associated with their systematic wearing. One of them is due to the paradoxical discrepancy between cases of the development of dry eye syndrome in users of these lenses and at the same time, sometimes occurring recommendations to actively prescribe SCLs for the treatment of this disease. The material below is devoted to a more detailed consideration of this problem.
First of all, issues related to the features of the functional interaction of SCL and SP are of great practical interest. It has now been proven that a contact lens placed behind the eyelids of a healthy person is “introduced” into the structure of the joint (Fig. 24) and divides it into two parts - pre- and sub-lens (Gufflon J., 1982).
As a result, the thinned lipid and mucin layers of the SP become more vulnerable to exo- and endogenous factors.
At the same time, SCL, like a “foreign body,” increases irritation of the reflexogenic zones of the cornea and conjunctiva and thus increases the volume of reflex tear production. In turn, an increase in the volume of the aqueous component of the joint venture stimulates an increase in the secretion of lipids and mucin, without which its stability will decrease. However, this compensatory process is possible only if the function of the glands that produce them is not impaired. If it begins to suffer, then first of all this affects the state of the lipid layer of the joint venture, which is subject to destruction.
As a result, the prelens SP breaks in certain areas and this process is accompanied by abundant precipitation of lipids onto the surface of the SCL. At the same time, the evaporation of moisture from the aqueous layer of the joint venture increases, which leads to its thinning and instability.
Then, if adequate corrective therapeutic measures are not taken, the pathological process may develop further. At first, its dynamics consist of an increase in reflex lacrimation, which, over a period of time, compensates for the loss of tear fluid volume due to evaporation.
This dynamic balance is then disrupted due to functional depletion of the continuously stimulated lacrimal glands. This is facilitated by the suppression of tear production that sometimes occurs due to diseases that we have already discussed in the second section of the book (undiagnosed dry eye syndrome), as well as against the background of long-term systemic use of a number of pharmacological drugs (see Appendix 1).
A decrease in tear production leads to an increase in the osmolarity of the joint venture. The latter factor contributes not only to the development of secondary dehydration of corneal and conjunctival epithelial cells, but also to a decrease in moisture content in the SCL.
Simultaneously with the decrease in the volume of the SG, the mobility of the SCL on the eye also decreases, which contributes to the accumulation of lumps of mucus and degenerated epithelial cells under it, which is already characteristic of the involvement of the mucin layer of the SG in the pathological process. The maximum changes are observed at the edge of the SCL, at 3 and 9 o'clock. In addition, the outer surface of the lens is gradually covered with protein and mucous deposits. In parallel, metabolic disorders of the corneal epithelium also occur.
Thus, SCL placed on the cornea is capable, under certain conditions, of disrupting the structure and stability of the joint, leading to changes that contribute to the development of the symptomatic dry eye disease already discussed above. These conditions typically occur in patients with meibomian gland dysfunction, of any type; that is, with both hypo- and hypersecretion of lipids, as well as with reduced tear production and impaired stability of the joint venture.
The situation is noticeably aggravated if the surface of the SCL has any defects, even the most minimal ones. The mechanism of disruption of the structure of the lipid layer of the joint venture during hypofunction of the meibomian glands has already been discussed above. As for their hyperfunction, in this case excess lipids are combined (including by covalent bonds) with polar mucin molecules.
As a result, small mucin-lipid particles, insoluble in the aqueous layer of the lens, are formed, which float in the thickness of the pre-lens and sub-lens lens and are displaced during the blinking movements of the eyelids. At the same time, the formation of “dry spots” occurs on the surface of the SCL and cornea. As a result, such a pronounced disruption of the structure of the lipid layer of the joint significantly increases the evaporation of the joint, which quickly becomes thinner even with satisfactory function of the lacrimal glands.
As already discussed above, a decrease in tear production with impaired stability of the joint due to inhibition of mucin secretion is characteristic, in particular, of women in the menopausal period. Their situation becomes more complicated after cataract extraction with aphakia correction with a contact lens.
Thus, from the above data it is clear that the selection. SCL should be accompanied by a balanced assessment of the state of tear production and stability of the joint in each individual patient. Unfortunately, in practice this usually does not happen and therefore there is always a potential danger of either stimulating the development of symptomatic dry eye syndrome or aggravating an existing but undiagnosed disease of this type.
In particular, of the 57 patients we examined (together with Kononov V.M.), wearing SCLs made of hydroxyethyl methacrylate, good tolerability of the lenses was noted in 50 (87.7%) of them. However, some patients (4; 8.0%) systematically used their humidifiers as installations. Seven people presented complaints typical of patients suffering from symptomatic dry eye syndrome: moderate photophobia, sensation of a “foreign body” in the conjunctival cavity, “burning” and “stinging” in the eye, poor tolerance to wind, conditioned air, smoke, etc., deterioration of visual performance in the evening, fluctuations in visual acuity.
These complaints persistently persisted even in cases where patients constantly installed drugs into the conjunctival cavity designed to increase the stability of the joint. In four of them, examined 30-60 minutes after removal of the CL, a significant decrease in the stability of the SP (up to 5.6 + 1.2 s) and a slight decrease in the amount of main tear production (up to 9.8 + 2.0 mm) were found. The value of reflex tear secretion turned out to be even slightly increased (up to 13.4+5.1 mm). The data obtained are typical for symptomatic dry eye syndrome associated with a predominant disruption of the structure of the tear film.
Numerous cases of intolerance to SCLs, noted both immediately after their placement and in the long term against the background of systematic wearing, naturally raise the question of the possibilities of correcting this condition. It is known that, in principle, it can be stopped by instilling into the conjunctival cavity solutions that moisturize the lens, offered by CL manufacturers, as well as drugs that increase the stability of the joint lens (the so-called “artificial tears”, discussed in detail in section 6 of the book).
However, due to the fact that most of them contain toxic preservatives (chlorobutanol, benzalkonium chloride, etc.), we turned to polymer solutions that are widely available in the clinic, similar in formulation, but free from harmful impurities. Polyglucin, which is based on low molecular weight 6% dextran, has proven itself well in this capacity.
It is advisable to instill it directly onto the contact lens. The frequency of instillations is determined individually. In this case, the indication for the next instillation of the drug is the resumption of subjective discomfort, the symptoms of which are indicated above. As a result of long-term observation (3-5 years) of 15 such patients (all wore hypolan SCL), it was found that in 9 of them, systematic distillation of polyglucin contributed to the complete disappearance of symptoms of symptomatic dry eye syndrome, and in 6 - partial disappearance.
Having considered the main causes and mechanism of occurrence of symptomatic dry eye syndrome due to wearing SCLs, we should turn to another aspect of the same problem - the use of SCLs for the treatment of patients with dry eye syndrome.
It has been established that wearing a hydrophilic CL with a moisture content of 60-85% allows you to protect the covered cornea from irritation by blinking movements of the eyelids and external artificial factors. In other words, in this case it serves as a kind of moistened “bandage”, very effective for Corneal erosions caused by mechanical or burn trauma, irritation of the eyeball by the tips of suture threads, etc. states.
Since the attitude towards the prescription of SCL for the treatment of patients with dry eye syndrome according to the literature is very ambiguous, we (together with Gladkikh A.F. and Kononov V.M.) observed 34 patients using SCL made of hydroxyethyl methacrylate and Almacon.
Their results are presented in Table 7. It shows that in all patients with dry eye syndrome, which developed due to a decrease in the production of tears and mucins (menopausal syndrome and Sjögren's syndrome), wearing SCLs led to an even greater decrease in the stability of the spinal cord (the differences, however, are not statistically significant; p>0.05) and the appearance of pronounced signs of CL intolerance. These phenomena in all 3 patients with Sjögren's syndrome and in 3 out of 7 patients with menopausal syndrome served as the reason for their voluntary refusal to further wear SCLs.
There were no significant dynamics in the functional indicators of tear production and stability of the SP when wearing SCLs in patients with pathology of the corneal surface caused by cicatricial changes after mechanical injuries and burns (see Table 7).
Thus, in patients with dry eye syndrome caused by a decrease in the production of components of the joint and a violation of its structure, but not associated with the pathology of the outer membrane of the corneal epithelium (they make up the bulk of patients with dry eye syndrome), placement of SCL significantly worsens the clinical course of the underlying disease.
It should be emphasized that the examination of patients both before placing an SCL and while wearing it should include the methods already discussed in the 4th section of the book, allowing for a comprehensive assessment of the state of tear production and the stability of the joint.
As an example, we present observation data on a patient with symptomatic dry eye syndrome that developed due to wearing an SCL from a hypolan.
Patient S, 32 years old, having put on contact lenses, constantly experienced a feeling of “discomfort” in the eye (sensation of a “foreign body”, “burning”, etc.), intensifying in air-conditioned rooms, when working with a computer monitor, as well as in evening time.
Purposeful collection of anamnesis revealed that the patient had periodically observed similar phenomena before, but when wearing SCLs, they significantly intensified. Upon examination: the position and mobility of the SCL on the eye are correct; after removing the lens, there is a slight injection and swelling of the conjunctiva, the cornea is intact.
Results of the Functional study: stability of SP-7s, amount of total tear production - 16mm, main - 6mm, reflex - 10mm. Based on the examination results, symptomatic dry eye syndrome was diagnosed, caused by a combination of a deficiency of the main tear production and a decrease in the stability of the joint with microsigns of xerosis. Prescribing polyglucin instillations to the patient while wearing SCLs made it possible to increase the tolerability of contact lenses.
As our own studies and those carried out by some other authors have shown, the results of functional studies and targeted history taking make it possible to accurately identify individuals at risk of poor tolerability of SCL. They make up a whole group.
It includes patients with the following pathologies:
- Sjogren's syndrome;
- dysfunction of Becher's glands of menopausal origin;
- endocrine ophthalmopathy;
- clinical forms of dry eye syndrome caused by a decrease in the main tear production (less than 7 mm);
- dysfunction of the meibomian glands (especially the type of meibomian blepharitis);
- paralytic lagophthalmos or incomplete closure of the palpebral fissure of another origin;
- a pronounced decrease in tactile sensitivity of the cornea.
A certain risk in this aspect also arises in cases where the patient must constantly remain in conditions associated with exposure to a number of unfavorable factors on the eye that provoke the development of symptomatic dry eye syndrome: wind, dry conditioned air, dusty premises, smog, etc.
Long-term use by the subject of a number of pharmacological agents that inhibit tear production is also important (see Appendix). The doctor's caution should also be caused by the patient's history of a tendency to recurrent conjunctivitis and keratoconjunctivitis.
The signs listed above are not absolute for making a decision on refusing to select SCLs for one or another patient or canceling their wearing, but only allow, with a certain degree of probability, to predict the development or worsening of the existing dry eye syndrome and guide the doctor to prescribe installations of lens humidifiers.
We found that in 19 out of 30 (63.3%) patients with the above prognostic signs of poor tolerability of CL, the clinical manifestations of the latter significantly decreased against the background of systematic instillation of polyglucin into each eye.
Thus, the problem of the relationship between the use of SCL and dry eye syndrome requires individual consideration in each specific case. Clinical and pathogenetic forms of dry eye syndrome associated with a lack of tear production (both of its components are equally important) and increased evaporation of the joint, as a rule, are aggravated while wearing SCL.
In addition, in case of dry eye syndrome associated with pathology of the outer epithelial membrane of the cornea, in most cases, MCLs turn out to be a very indifferent therapeutic agent and are also not indicated. It is possible that the development of more effective SCL humidifiers will further expand the indications for the prescription of contact lenses for dry eye syndrome. At the moment, it is possible to improve the tolerability of SCLs by installing a polyglucin solution directly onto the lens according to an individually selected scheme.
Moisturizing lenses - features of choice
An excellent solution for eliminating dry eyes are moisturizing lenses. Today there are quite a lot of them in the line - choosing the ideal option will not be a problem. The most popular gyrogel lenses are discussed in the article.
1-Day Acuvue Oasys with HydraLuxe
Acuvue's comfortable one-day lens options allow you to maintain an optimal level of eye hydration. HydraLuxe technology protects your eyes all day long because... Gives lenses the properties of natural tears. They are made on the basis of senofilcon A, a unique polymer. Guarantees a clear picture at any time of the day. These are some of the best daily lenses. Estimated at 1500 rubles.
According to reviews, they are as comfortable as possible and invisible in use.
Dailies Total 1
New generation contact lenses – this is what Dailies call this version of lenses. They are recommended for beginners, people suffering from dryness, those with sensitive eyes, and those who experience discomfort when wearing conventional options. These lenses distribute liquid correctly, they allow oxygen to pass through perfectly, and the surface is made without the use of silicones. They are comfortable all day long.
Price per set – from 1650 rubles.
Reviews on thematic sites confirm that they are quite good. They are convenient both on vacation and while traveling. Many people note that they cannot be called the most ideal, but in general they are quite good.
Acuvue Oasys with Hydraclear Plus
Long-term wearing features high comfort of use. They are made on the basis of hydrogel - a soft material. They do not interfere with blinking and are not felt during the day. Designed for use within 2 weeks. They protect well from ultraviolet radiation, blocking rays. The eyes breathe freely in them, redness is excluded. The cost of these starts from 1050 rubles.
According to reviews, this is an ideal option for optimal and comfortable vision. Many do not part with them not only for years, but for decades.
Biofinity
Cost from 1290 rubles. They are called innovative. Aquaform technology provides higher hydration and oxygen supply. Made from silicone hydrogel. According to reviews, they are very cool and imperceptible. They are called the best in their segment.
Air Optix Night & Day Aqua
Cost from 1300 rubles. Made from silicone hydrogel. Designed for daytime wear. But can be used continuously for 30 days. Many in their reviews call them favorite and ideal. And the fact that you can wear them for a whole month without taking them off and feel comfortable gives them a 100-point head start. Alcon colored lenses are also very comfortable to wear.
The following recommendations will help protect your eyes from dryness caused by wearing lenses:
If you constantly feel dryness and discomfort in your eyes when wearing lenses, they should be removed from your eyes and consult an ophthalmologist. The clinic will prescribe the necessary tests and examinations that will help determine the exact cause of dry mucous membranes. Depending on the results of the study, the doctor will advise what needs to be done to eliminate dryness of the corneal epithelium. Usually, to prevent contact optics from drying out your eyes, it is enough to adhere to the following rules:
Hygiene
Do not forget about the hygiene procedures required for optical products. Dry corneas are often caused by neglecting lens care. For people who do not want to clean an optical product, the use of disposable models will be safe for the health of the mucous membrane. Since daily lenses do not need to be disinfected and cleaned, unlike contact lenses intended for long-term use.
To clean scheduled replacement products, you need to use special solutions. They destroy bacteria and viruses, and also moisturize the lenses and remove deposits and dirt from their surface. Products that protect against tear fluid evaporation and moisturizing lenses Biotrue, Unica Sensitive, Maxima, PureVision have proven themselves well;
Contact lens replacement time
You should remember the timing of replacement and the mode of use of contact lenses. If you do not take into account the time interval during which you are allowed to wear optical products without removing them, dry mucous membranes will appear quite quickly. The same thing will happen if you wear contact correction products with a short service life for a long time. Timely replacement of old optical devices with new ones prevents the development of dryness and damage to the mucous membrane. The shelf life of these products depends on the processing methods of the material from which they are made and their characteristics. When wearing expired vision correction products, their resistance to protein and fat deposits decreases and infectious inflammation of the mucous membrane may occur.
Moisturizers
Apply eye moisturizers. If vision correction products are selected correctly, hygiene rules and wearing conditions are followed, lenses are not the cause of corneal dryness. The feeling of dry eyes may appear due to lack of sleep, eye fatigue, or after sitting at the computer for a long time. Special eye drops, gels and emulsions effectively combat discomfort caused by dry mucous membranes. They eliminate unpleasant symptoms and restore moisture to the surface of the eye. It is better to purchase moisturizing drops that can be used without removing correction products. Products that restore the functioning of the lacrimal glands: Adria Relax, Pro Active, VizoTeque Pure Crystal, Optimed Drops, Systane Ultra, cope well with the problem of dryness. When choosing drops, you should definitely consult with an ophthalmologist, because only he can choose the care products that are right for you.