The human eye is a complex optical lens. It consists of many structures, each of which performs its assigned function.
This technically sophisticated design works seamlessly to produce crisp color images.
As you work hard, depending on external and internal factors, disruptions occur in the system of perception, processing or reproduction of information. Myopia is considered one of the perception disorders. This is a common pathology that requires long-term or permanent vision correction.
What is myopia
Myopia, or myopia, is ametropia caused by a violation of the focus of light beams. The intersection of electromagnetic waves from objects is localized not on the retina, but in front of it. Scattered rays pass through the retina. The pathology is characterized by clear vision near and blurred vision at a distance.
Two systems are responsible for spatial vision: refraction and accommodation. Refraction is responsible for the refraction of light emanating from surrounding objects. The rays are refracted when passing through the transparent media of the eye - the cornea, anterior chamber fluid, lens, vitreous body. Normally, refracted beams of light are focused on the retina, then the signals are converted into a nerve impulse and transmitted to the visual analyzers of the brain through the optic nerve. The response is the appearance of the final image and its reproduction.
With myopia, the point of intersection of light rays does not reach the retina. The focus is localized in front of her. Short rays from nearby objects still reach the retina. Therefore, myopic people see well at a distance of no more than 100 meters. The further the distance from the target, the worse it is caught by the eye.
Accommodation allows you to “tune” the eye to different vision distances. The adaptation mechanism of the eye is based on changes in the curvature of the lens. When looking into the distance, the contraction of the ciliary muscle decreases, the ligament of Zinn tightens, and the lens flattens. This reduces its refractive activity. This allows long light waves to reach the retina.
In near vision the opposite situation occurs. The ciliary muscle contracts, relaxing the ligament of Zinn. At the same time, the lens becomes habitually convex, increasing its refractive power. Light beams are refracted with greater force, which prevents the focus from “flying” beyond the retina and being localized directly on it.
Myopia
Myopia (syn. myopia) is one of the types of refractive error of the eye, in which parallel rays of light entering the eye, after refraction, converge in focus not on the retina, but in front of it. The concept of “myopia” is due to the fact that with this anomaly the object in question is clearly visible only at a close distance. Another name for myopia (Greek myo I close, I squint my eyes) is due to the fact that people with such an anomaly squint their eyes in order to better see distant objects. This helps produce clearer images on the retina.
With normal, commensurate emmetropic refraction (see Emmetropia), parallel rays of light entering the eye, after refraction, converge in focus on the retina; with B. this does not happen. Parallel rays, after refraction in a myopic eye, unite at a focus - at some point in front of the retina (Fig. 1); Consequently, the main rear focal length turns out to be relatively shorter than the length of the eyeball. This may depend either on the fact that the refractive system of the eye is relatively strong (the so-called refractive power), or on the fact that the longitudinal (anterior-posterior) axis of the eye is too large compared to its refractive power (the so-called axial power) .). Refractive B. is practically of little importance, but in the clinic we have to deal with hl. arr. with axial B.
| Rice. The course of rays in a myopic eye: 1 - parallel rays (emanating from distant objects) are focused in front of the retina; 2 - diverging rays (emanating from nearby objects) are focused on the retina. | ||
According to some authors (E. Zh. Tron), a significant number of cases of B. should be classified as so-called. combinational B., in which both the length of the axis of the eye and the refractive power do not exceed the values found in emmetropia. But both of these factors are combined in such a way that the result is B.; it should be noted that Raman B. usually includes cases with a relatively low degree of this type of refractive error.
If parallel rays emanating from infinitely distant objects are refracted in a myopic eye in such a way that their focus is in front of the retina, then as the object approaches the eye the rays will gradually take an increasingly divergent direction, and the focus after their refraction in such an eye it will move closer and closer to the retina. Finally, with a known position of the object, the degree of divergence of the rays coming from it will be such that the focus just falls on the retina (Fig. 2), and a clear, distinct image of the object is formed on the retina for the first time. This is a further point of clear vision (see). All objects lying beyond this point are seen by the myopic eye in circles of light scattering, that is, unclearly. The position of this point determines the so-called. degree B., which is usually expressed in diopters. If the further point of clear vision is at a distance of 1 m in front of the eye, then this will correspond to a B. of 1.0 diopters. When this point is positioned at a distance of 50 cm from the eye, B. will be equal to 2.0 diopters, at a distance of 25 cm - 4.0 diopters, etc. Thus, the higher the degree of B., the shorter the distance, within which the myopic eye is able to see clearly.
When an object approaches the eye closer than the further point of clear vision of a given eye, the rays emanating from the object take on such a degree of divergence that they would have to converge only behind the retina.
In fact, this does not happen, because accommodation is switched on and the rays are refracted more strongly and converged on the retina. The point closest to the eye, the rays from the cut can still converge in focus on the retina and the edges can be clearly visible at the maximum voltage of accommodation, is called the closest point of clear vision (see). The distance between the further and the nearest points of clear vision is the distance within which the myopic eye can see well. In most cases, this distance is not large and depends on ch. arr. on the degree of B. (the higher the B., the shorter this distance), as well as on the strength of accommodation. The last factor, however, plays almost no role with B. at 3.0-4.0 diopters, since the further point of clear vision of such eyes lies at a distance of 33-25 cm in front of the eye, that is, it is located from the eye at the usual level. the average, most convenient working distance, and in this case there is no need for the eye to enhance its refraction by turning on accommodation.
In order for a myopic eye to clearly see distant objects from which parallel (or close to them) rays come, these rays must be made divergent. This can be achieved by using appropriate diverging lenses. A lens that gives the degree of divergence of parallel rays corresponds to their divergence from a further point of clear vision of a given eye, and determines its degree B. Such a lens has a focal length equal to the distance from the eye of a further point of clear vision. Thus, on the one hand, the degree of B. is determined by the position of the further point of clear vision, and on the other hand, by the refractive power of the lens correcting B., one can judge the position of the further point of clear vision of a given eye. The refractive power of the lens (in diopters) shows how much the refraction of a myopic eye should be reduced. These diverging lenses are used to correct (correct) myopia.
Since, according to the conditions of their vision, myopic people are usually forced to hold the object in question close to their eyes, the eyes converge strongly (see Convergence of the eyes). Due to the presence of physiol. connection between convergence and accommodation of the eye (see) in myopic people there can sometimes be a special state of involuntary long-term excessive strain of accommodation (the so-called spasm of accommodation), which further enhances the refractive ability of the eye, i.e. makes it seem even more myopic, than it is (pseudomyopia). With strong, prolonged convergence, the load on the internal rectus muscles of the eyes increases; this circumstance can lead to symptoms of fatigue, muscle fatigue (so-called muscular asthenopia), accompanied by a feeling of aching eyes, pain in the eye sockets, and headache. In this case, it is necessary to interrupt the work associated with the tension of accommodation. The phenomena of muscular asthenopia disappear if one eye is closed, because when using only one eye, convergence disappears.
Due to the fact that myopic people must converge strongly, but do not need accommodation, physiol. relationship between these two functions. The muscular convergence apparatus, not supported by the necessary impulse from accommodation and forced, in addition, to work hard, becomes exhausted, binocular vision is upset, first only temporarily, and then for a long time and persistently. Monocular vision is established, as a result of which the eye, excluded from the act of binocular fixation, deviates outward, i.e. concomitant divergent strabismus develops.
Distance visual acuity in myopic people is always below normal, however, with the help of appropriate diverging lenses that correct vision, visual acuity can be significantly improved, especially with weak and moderate degrees of vision. With a higher degree of vision (above 6.0 diopters), visual acuity as a result of correction with lenses, it still remains below normal, and with B. above 10.0 diopters, it is almost impossible to achieve normal visual acuity with correction. This is due to changes in the fundus, most pronounced with high B.
Etiology. Many conflicting opinions have been expressed on the issue of the origin and reasons for the development of B. The starting point for the construction of various theories of B. was a number of firmly established facts. These include, first of all, the fact that children are almost always born farsighted. Congenital B., diagnosed from the first days of life, is a very rare phenomenon. In the vast majority of cases, myopia begins to develop during school years—in the lower grades, there are fewer myopic children and the degree is p. theirs is lower than that of older school children. There are more myopic people in those industries and workshops where they have to carry out intense work for a long time at a close distance from their eyes. All these indisputable facts formed the basis for the construction of the theory of “school biology”, or “working vision”, which recognized work at a distance close to the eyes as the immediate cause of the development of vision. A number of authors put forward the factor of heredity as the main reason for the development of B. Proponents of the hereditary theory of the origin of B. (M.I. Averbakh and others) referred to the fact that in the same family (under the same conditions) some children develop B.g. and others do not, that the eyes identical twins usually show striking similarities in refraction, etc.
Without denying the role of heredity in the origin of B, it must still be said that the recognition of environmental factors as being of decisive importance in the formation of clinical refraction of the eye, in particular B., in the process of ontogenesis is most consistent with modern scientific views. According to some authors (E. S. Avetisov and others), the main reason for the development of B. (at least weak and moderate degrees) is the weakness of the ciliary muscle, resulting from unfavorable conditions for visual work, and in connection with this insufficiency accommodation, and the consistent lengthening of the anterior-posterior axis of the eyeball can be considered as a kind of adaptive, compensatory act aimed at ensuring the possibility of long-term work at a distance close to the eyes.
Clinical picture. All encountered cases of B. are usually divided according to their degree into 3 groups: weak degree - up to 3.0 diopters, moderate degree - from 3.0 to 6.0 diopters, and high degree - from 6.0 diopters and above. Occasionally there are cases of B. up to 20.0-30.0 diopters and even higher. One should distinguish from high B. severe, malignant, or progressive B., in which there are certain complications at the bottom of the eye, in its membranes. Progressive B. always refers to axial, and not refractive. Since in general the clinic has to deal primarily with axial vision, it should be borne in mind that lengthening the axis of the eye by 1 mm entails an increase in refraction by 3.0 diopters, or, what is the same, an increase in refraction by 1.0 diopter corresponds to an extension of the eye axis by V3 mm.
Among the total number of myopic people, the most common cases are weak and moderate degrees of myopia; more than half of the known cases are classified as combined myopia. B. of high degrees, progressive, accompanied by various complications, is interpreted as a pathological condition, which may be caused by congenital inferiority of the organ or acquired under unfavorable external conditions, as a result of which it became possible to lengthen the anterior-posterior axis of the eye with the subsequent development of degenerative-atrophic changes in its tissues and membranes.
An extremely common symptom of B. are the so-called. “flying floaters”, visible to the patient in the form of small grayish clouds that move when the eyeball moves.
With B. of medium and especially high degrees, the appearance of the eyes has certain characteristic features: the eyeballs stand forward somewhat, the palpebral fissure appears wider than normal, the anterior chamber of the eye is deeper than normal, the pupil is of a larger diameter. During an ophthalmoscopic examination of the fundus of the eye, even with weak degrees of B., as a result of relative stretching and atrophy of the membranes of the eye, in particular the choroid, the so-called optic disc is often observed near the optic nerve head. posterior cone, or posterior staphyloma, and at high degrees of B. - true posterior staphyloma (color table, article 489, Fig. 1 and: 4). According to the mechanism of development, the posterior cone is called distraction, i.e., a cone from stretching.
In mild cases, ophthalmoscopy reveals a white or yellowish crescent on the temporal side of the optic nerve head. In more severe cases, a gradually progressive degenerative-atrophic process occurs in the choroid and in the retina around the optic nerve, sometimes covering a large area, including the most functionally (visually) important area of the macula. A similar process can also occur in the peripheral parts of the fundus, where its development is, however, less important for vision function. In case of lesions in the area of the macula - the so-called. myopic maculitis, or central myopic chorioretiitis, due to rupture of small blood vessels, repeated hemorrhages into the retina and even into the vitreous are often observed, and hemorrhages into the retinal tissue often do not resolve completely and in their place a grayish or even black color forms (due to subsequent pigmentation) spot (Fuchs' black spot) (color Fig. 2 and 3). Vision suffers greatly with this complication. With these changes in the retina as a result of displacement of the nervous elements, metamorphopsia is often observed, i.e. seeing objects in a distorted form.
| Myopia. Fig.1. Rear double cone. Rice. 2. Posterior staphyloma and central choriotetinitis with hemorrhage. Rice. 3. Central choriotetinitis with hemorrhages. Rice. 4. True posterior staphyloma. | ||
The most severe complication with B. is retinal detachment (see). This complication, which usually occurs only in moderate and high degrees of B., sharply reduces vision and can lead to complete blindness if surgery is not performed in a timely manner, which will ensure reattachment of the detached retina. Any conservative treatment is usually unsuccessful.
B.'s diagnosis is based on objective research data through the so-called. shadow test (see Skiascopy) and with the help of special devices - refractometers (see Refractometry of the eye), as well as on the basis of subjective testimony of the subject in the process of determining visual acuity using corrective lenses (see Visual acuity).
Treatment. The vast majority of cases of B. require only correction with glasses; progressive, malignant B., in addition to correction, requires systematic general and local treatment. In persons with a malignant course of B., especially in children, signs of general diseases of the body are often found; with atherosclerosis, hypertension, menopause, etc. B. takes an unfavorable course. These diseases are aggravating factors that can lead to a number of complications in the myopic eye.
The task of B.'s correction is, first of all, to improve the vision of the myopic eye through optical glasses (see Glasses) and thereby bring it, or at least bring it closer, to the vision conditions of the emmetropic eye.
Most authors believe that glasses that completely correct B should be prescribed. Complete correction provides not only the highest possible visual acuity for a given eye, but also restores the correct relationship between convergence and accommodation, thereby favorably influencing many physiol. processes in the eye. When working with an object that is at a close distance from the eyes, myopic people of weak and medium degrees may not use glasses or they are prescribed glasses 1.0-2.0 diopters weaker than those required for distance.
Speaking about the complete correction of B., it should, however, be noted that persons suffering from B. cannot always tolerate full correction with glasses when worn constantly. Children and adolescents, as a rule, easily tolerate full correction and successfully use it with both weak and moderate degrees of B. If glasses are prescribed for the first time at an older age and with B. not weak degrees, then glasses for distance are completely corrective glasses may be well tolerated, but using these glasses for exercise can be difficult. This is due to the fact that with full correction for close-range activities, accommodation must be turned on. The eyes of young people with a good amount of accommodation reach the required degree of accommodation tension without any effort. Young people can work for a long time without the unpleasant phenomena of eye fatigue. In older myopic people, the amount of accommodation is smaller, and therefore they often cannot tolerate full near correction. In such cases, glasses are prescribed, which do not completely correct B. At high degrees of B. (above 6.0 diopters), full correction is sometimes poorly tolerated; even for distance vision, it is necessary to prescribe those glasses that are practically tolerated and, if possible, provide satisfactory visual acuity. Glasses that do not fully correct high vision are most often used simultaneously for distance and close-range activities. In some cases, it is better to have glasses for distance, which, if possible, completely correct vision, and glasses 2.0-3.0 diopters weaker for near work.
When prescribing glasses to myopic people, it is often necessary to take into account their existing weakness of the internal rectus muscles and to decenter the glasses (increase the distance between the centers of the glasses by 1-2 mm) in order to facilitate visual work at close range. With such decentration, the prismatic action of the glasses facilitates the work of the internal rectus muscles of the eye. Corrective glasses with scattering action are most often manufactured in the form of convex-concave (so-called menisci, punctal glasses, etc.). Their optical effect is more perfect than that of previously used biconcave glasses. Convex-concave glasses more completely eliminate the so-called. astigmatism of oblique rays is corrected not only by a stationary eye, but also by making certain movements with changing directions of gaze.
With high B. and a significant decrease in visual acuity (below 0.2 with correction), ordinary glasses often do not provide adequate improvement in vision, especially since complete correction in these cases is poorly tolerated; increase visual acuity with the help of the so-called. telescopic glasses. They have the appearance of small binoculars worn like glasses. The telescopic system is an individually selected combination of a diverging lens (as an eyepiece) with a collecting lens (as an objective) - similar to the principle of theater binoculars or a Galilean telescope. A feature of such glasses is the ability to obtain full correction of vision, which ensures correct focusing of the image on the retina and helps improve vision. In addition, the telescopic system provides a certain magnification (approximately 1.7 times) of the image of objects on the retina (which ordinary corrective glass does not provide), which also creates more favorable conditions for vision. The negative side of telescopic glasses is the limitation of the field of view when using them; In addition, they are bulky. When using telescopic glasses for near work, a special attachment (i.e., an additional lens) is required; practically only one eye works (monocular vision).
With the help of contact lenses worn directly on the front surface of the eyeball (behind the eyelids), it is possible to improve vision correction, especially at high levels, to a greater extent than with spectacle glasses.
When treating B., treatment should be carried out by prof. measures that, to one degree or another, delay the development and progression of B. For the treatment of various complications (degenerative-atrophic changes in the membranes of a distended myopic eye) occurring in B., agents are used that promote the resorption of decay products of damaged tissues and stimulate the visual-nervous elements, damaged to one degree or another, but capable of functioning at a lower level than normal.
As absorbable agents of general action, various iodine preparations are used orally in small doses. Locally, in the form of eye drops, 1 - 10% dionine solutions are widely used. Dionin in the form of a 2-5% solution is also used for subconjunctival injections. A 3-5% solution of table salt, 0.5 ml, is also injected under the conjunctiva. Injection of oxygen under the conjunctiva (so-called oxygen therapy) is practiced.
As a stimulant, subcutaneous injections of vitamin Bj (5% solution) 1 ml are prescribed for a course of up to 25-30 injections. Treatment with biogenic stimulants (according to Filatov) in the form of injections of aloe extract, placenta, FiBS, peloid distillate (1-2 ml daily; for a course of 30-45 injections, repeated after 2-3 months; 4 courses per year) is widely used. . V. P. Filatov put forward the idea of the need for early and systematic use of tissue therapy for the purpose of not only treating complicated B., but also as an event that, in his opinion, can, to one degree or another, prevent the development and progression of B.
If you are prone to hemorrhages in the membranes of the eye and in the vitreous body, you should resort to the prescription of antihemorrhagic drugs (vitamins C and P, rutin, etc.).
In the 60-70s of the 20th century, reports appeared in foreign and domestic literature about attempts to surgically stop the progressive stretching of the sclera of a myopic eye and thus avoid the progression of the pathological process in the retina. For these purposes, cadaveric fascia lata and cadaveric sclera were commonly used.
Forecast. With mild and moderate B., appropriate correction allows you to maintain your ability to work. With B. of moderate degree with a tendency to progression and high degree, the prognosis mainly depends on possible complications. The prognosis for malignant B. is unfavorable, in which pathological changes in the fundus often tend to progress.
Prevention. The correct point of view on the issue of B.'s genesis is essential for organizing the fight against B. and preventing its development. Recognition of environmental factors as being of primary importance for B.’s development provides the most serious grounds for the entire set of dignity. gig. activities carried out to prevent the development and progression of B. Among these activities, the implementation of which is especially important in relation to school-age children, the following should be indicated. Excessive proximity of the object of study to the eyes, which is also associated with a strong tilt of the head forward (down), should be limited; it is necessary to take care of sufficient and rational natural and artificial lighting in schools and work areas, the arrangement of comfortable desks and benches, and the correct position of the student’s torso during classes. The quality of printing of school textbooks is of great importance (see Vision, hygiene).
Persons with complicated B. should avoid anything that can cause a rush of blood to the head; It is advisable to protect your head from direct sunlight; In bright light, you should use tinted glasses (corrective filters) of medium intensity. Such persons should, if possible, avoid physical activity. tension and sudden movements in order to protect against possible hemorrhages and retinal detachment.
The operating mode is of great importance; classes should be organized in such a way that for every 40-45 minutes. visual work required 10-15 minutes. complete rest for the eyes. What is important is rational and well-thought-out lighting, sufficient in strength and well illuminating the workplace and subject matter, but leaving the head and face in the shadow. You should not lean close to the subject of study (if possible, no closer than 30-35 cm). Proper posture, ensuring normal breathing and blood circulation, should be one of the conditions necessary for the normal development of a growing organism.
The question often arises about choosing a profession for a myopic person graduating from high school, and with this question they often seek advice from an ophthalmologist. When choosing a profession, myopic young people should give preference to specialties and those branches of labor where the visual and physical. the load is lighter where there are fewer demands on vision.
Persons with progressive B. and changes in the fundus of the eyes require a gentle working regime (limitation of the working day). However, complete refusal to work in most cases does not seem advisable; transition to disability and complete abandonment of the usual profession. work does not at all guarantee, as experience shows, stopping the process or preventing the disease of the other eye if one is affected. This issue, very serious from the point of view of labor expertise, should be resolved individually; in each individual case it is necessary to take into account not only the condition of the eyes and the nature of the profession, but also the general condition of the body.
Some of the complications caused by B. may require surgical treatment. Surgical treatment is indicated for retinal detachment. Surgical treatment must be resorted to in order to remove complicated cataracts, which often develop in eyes with severe myopia.
| Krasnov M.L. |
⇐ Go to the main page of the site ⇐ | ⇑ Return to top of page ⇑ | Ordo Deus Library ⇒ ⇒ |
⇐ Blepharitis | ⇓ Complete body of knowledge. Volume one A. ⇓ |
Classification
First of all, it is necessary to understand the concepts of true and false myopia. True myopia develops in the presence of pathology in the refractive and/or accommodative function of the eye, or external causes (trauma, neoplasm). Without correction, visual impairment progresses. False myopia, or spasm of accommodation, occurs with prolonged strain of accommodation. When the ciliary muscle is contracted for several hours, it does not have time to relax when looking into the distance. The lens retains its convex shape. In this case, the eyes do not focus properly, and the person sees a fuzzy picture.
This condition often develops with prolonged viewing of TV, working at a computer, or disruption of sleep and wakefulness. The accommodation spasm goes away after rest. But frequent occurrences of false myopia and regular adherence to risk factors lead to the progression of pathology and the development of true myopia.
There are congenital and acquired myopia. Congenital myopia is hereditary. If one of the parents suffers from myopia, then with a 50% chance his child will inherit the disease. With both myopic parents, the risk of developing myopia in a child increases to 75-100%. Acquired myopia is divided into early-acquired (in preschool children), acquired at school age and late-acquired.
There are several clinical criteria for the classification of all ametropia. Based on the sphericity of the optical system of the eye, conditionally spherical and aspheric myopia are distinguished. Aspheric ametropia occurs with astigmatism, while conditionally spherical ametropia occurs without it. According to the mechanism of development of the pathology, primary and secondary myopia are distinguished. According to the stability of the process - stationary and progressive. There are also complicated and uncomplicated forms of myopia.
Degrees
There are 3 degrees of myopia:
- 1st degree – weak;
- 2nd degree – average;
- 3rd degree – high.
With weak myopia, the optical power is deviated to -3.25 diopters. The average degree of deviation is up to -6.25 diopters. High myopia is characterized by a deviation of optical power above -6.25 diopters. Extreme myopia is defined as when the deviation is greater than -10.0 diopters. Currently, the boundaries of the degrees of myopia are blurred and are deprived of scientific argumentation. But still generally accepted norms of division remain to this day.
Types
The type of myopia depends on the structure of the eye that has undergone unhealthy changes. Axial (axial) myopia is spoken of when the length of the eyeball does not correspond to the axis of passage of light rays. This is a structural anomaly in the development of the eyeball - its excessively large anteroposterior size. In this case, there are no disturbances in the functioning of refraction and accommodation, the optical media of the eye function normally.
Lenticular (transient) myopia develops with somatic diseases and taking certain drugs of the sulfonamide group, corticosteroids, diuretics (chlorthalidone), and medications to lower blood pressure.
For example, with diabetes mellitus, the refractive function of the lens increases. Transient myopia is classified as false, since the manifestations disappear with the elimination of the etiological factor.
Change in corneal curvature. One of the reasons is keratoconus, when the cornea becomes cone-shaped instead of spherical due to inflammation. As the shape of the cornea changes, the refractive power increases.
Rate of progression
If visual acuity drops by 1 diopter per year or more, they speak of progressive myopia. Rapidly progressive myopia is almost impossible to correct; it is called malignant. This can lead to a rapid deterioration in health, complications and irreversible loss of vision.
False myopia
It turns out that myopia can be false. This occurs due to a decrease in visual acuity due to a spasm of accommodation. In this case, a person cannot clearly visualize objects far away or near him. During spasm, the eyeball becomes motionless and stops changing shape when focusing on distant/near objects due to a malfunction of the ciliary muscle. This condition is caused by overwork of the visual apparatus.
False myopia is a reversible phenomenon. But if overstrain of the visual apparatus occurs frequently, imaginary myopia becomes true. Therefore, you cannot delay your visit to the ophthalmologist. Particular attention should be paid to children under eight years of age, whose optical apparatus is in the formative stage. It is at an early age that you can get acquired myopia due to overexertion (reading, poor lighting in the workplace, incorrect posture, lack of vitamins).
False myopia, as a short-term phenomenon, can also appear while taking medications in the treatment of ophthalmological diseases. No therapy is required, as vision is restored after discontinuation of medications. There is also another form of false myopia, when the quality of vision is affected by several unfavorable factors: overwork, taking medications, and poor nutrition.
This pathology sometimes occurs in infants. Parents should closely monitor the development of the baby's visual system, because undetected pathology leads to strabismus and true myopia. At the age of three months, the baby already begins to react to toys, and the presence of pathology can be determined by his reaction. In older children, false myopia appears against the background of nervous experiences. You just need to show the child to a psychologist, and the problem will be resolved.
Causes
Hereditary predisposition remains a common cause of myopia. The reason that comes first in the development of acquired myopia is the anteroposterior size of the eyeball. Its value exceeds the length of the axis of refracted light. In this case, no organic disturbances of the transparent media of the eye are observed.
Additional groups of etiological factors:
- eye diseases - astigmatism, inflammatory diseases of the cornea with thickening and changes in the curvature of its wall, strabismus, clouding and dislocation of the lens, amblyopia;
- systemic diseases and injuries - traumatic brain injuries, diabetes, difficult pregnancy;
- deficiency of vitamins (A, B2), microelements - zinc, magnesium, copper;
- incorrect correction of previously identified myopia.
There are also risk factors, the combination of which provokes the development of the disease. These include:
- low illumination of the working and living areas;
- insufficient rest and sleep;
- long hours of continuous work at a computer monitor, watching TV, working with gadgets;
- primary weakness of accommodation;
- spasm of accommodation.
Causes of myopia
The causes of myopia or nearsightedness vary. Among them are two main ones:
- Genetic reason. Myopia is a hereditary disease; it is passed on to the child from parents genetically. If one or both parents are nearsighted, this markedly increases the likelihood that the child will inherit myopia. This is usually axial myopia, associated with the elongated shape of the eyeball.
- Poor visual hygiene. Many people do not care about eye health and are not familiar with the concept of visual hygiene. Therefore, they do not understand why myopia appears if you read lying down in semi-darkness or sit for hours at a computer without a break. But often these are the causes of myopia.
Symptoms
From the explanation of the mechanisms of development of myopia, the main manifestation of the disease is clear - relatively clear near vision with blurred distance vision. At first, patients do not pay due attention to this symptom. As the disease progresses, it causes you to squint your eyes when trying to look at an object or read an inscription from a distance. This is where the name of the pathology comes from – myopia (translated from Latin as “squinting the eye”).
Over time, additional symptoms appear:
- manifestation of visual impairment in the afternoon;
- headache, mainly in the temples;
- a burning sensation and discomfort in the eyes, lacrimation with prolonged strain on the visual apparatus;
- orientation in the dark decreases;
- the appearance of “flies” and “threads” before the eye speaks of destructive processes in the vitreous;
- the sclera becomes thinner, causing a blue color to appear (vessels become visible);
- the appearance of red spots and threads before the eyes is a common sign of retinal detachment.
Already the first signs of visual impairment require seeking specialized help.
Why is myopia dangerous?
It's not just about difficulty seeing or distinguishing distant objects. Myopia has a number of extremely unpleasant consequences. Nearsightedness.
- Frequent headaches.
- Decreased performance, difficulty learning.
- Reduced security level. A nearsighted person may not see a tram rushing towards him or, for example, an important road sign.
- Tearfulness, increased tendency to inflammation. This is due to the fact that the stretched tissues of the eyeball become thinner and irritation occurs on them more easily.
- High risk of developing other vision problems: retinal detachment, cataracts, glaucoma, myopic maculopathy (a condition in which the central region of the retina is damaged). All this can lead to blindness.
Diagnostics
Collecting complaints, asking about the onset, conditions of occurrence, chronic diseases and medications taken is a standard diagnostic kit when visiting a doctor. Next, based on the data obtained, the doctor begins instrumental diagnostics. In this case, it is necessary to confirm or exclude myopia, establish its degree, type, and complications.
Visual acuity is measured using tables with letters - visometry. This is the simplest and most important diagnostic method, allowing one to judge the degree of decrease in visual acuity.
The study of refraction and accommodation includes several methods. Refractometry is the measurement of refraction using an infrared beam reflected from the retina. Keratometry is based on the same mechanism: refraction is measured by reflecting light beams from the cornea. The condition for carrying out the method is the transparency of the refractive media.
Assessment of refraction using spectacle lenses to determine maximum visual acuity. A -0.5 diopter lens is placed in front of the patient's eye. In case of myopia, vision will immediately improve when visual acuity is set to 1 or lower. In ophthalmometry, images are projected onto the cornea.
The patient fixes his gaze on a certain point of the optical device. The doctor applies images to the cornea and, by controlling the device, achieves the merging of the spots into one. If the manipulation is successful, it means that the curvature of the cornea is normal. The presence and degree of astigmatism is diagnosed using ophthalmometry, refractometry and keratometry.
Skiascopy. The essence of the method is to observe the behavior of a light shadow passed through the pupil. The doctor shines a beam of light into the eye through the opening of the pupil. Light waves are reflected from the fundus of the eye and return. In this case, the doctor observes a red spot. If conjugation with the fundus does not occur, then the spot is black. When turning the device up and down, left and right, the researcher observes either a red or black pupil. The movement of the spot occurs along with the movement of the device.
With farsightedness, the further point of clear vision is behind the device, so the shadow will move in the same direction as the skiascope. The myopic eye focuses its gaze on a point between the eye and the device. In this case, the shadow from the light will move in the opposite direction from the device.
Using the proximetry method, the nearest and further points of vision are determined. A simple way is to use a ruler with an optotype (a table with letters for measuring visual acuity). The object is placed at a distance of 2-3 cm from the eye, the second eye is closed.
Move the table away until the patient sees the object. This is the closest point of vision. The point of further vision is determined using a lens of 3 diopters. When establishing a point, 3 diopters are added to the result obtained. In a similar way, using automated devices, absolute accommodation (of each eye separately with the opposite one closed) and relative (of both eyes) accommodation is determined.
Ergography – measurement of the work of the ciliary muscle. Loading the muscle at close range allows you to evaluate spasm or weakness of accommodation.
Additional methods for assessing visual functions include:
- fundus examination;
- visual field assessment;
- Ultrasound of the orbital region.
Degrees of myopia
Weak (1st degree myopia)
A characteristic sign of low myopia is squinting of the eyes when focusing on an object, fatigue during exercise, and frequent blinking. The disease is accompanied by photophobia and discomfort in the visual organs. Myopia of the 1st degree can develop over the years without causing any particular inconvenience. However, only an ophthalmologist can identify myopia at the initial stage; for this, viziometry is used - a test with a table of letters of different sizes.
Myopia differs from farsightedness in the way light rays are refracted: they are focused in front of the retina. With farsightedness, light refraction occurs behind the retina.
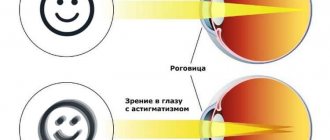
It should be remembered that myopia can be a manifestation of astigmatism, a more complex disease. With astigmatism, deformation of the corneal layer or the body of the lens occurs. If the pathology is not noticed in time and corrective measures are not taken, then the person will completely lose visual acuity over time. Astigmatism is diagnosed by an ophthalmologist using hardware technology. Average myopia uncomplicated by astigmatism is much easier to cure: the ophthalmologist will select a set of eye exercises and a complex of vitamins.
Average (myopia 2 degrees)
Myopia of the 2nd degree is manifested by a decrease in the quality of visualization at a distance of 2-3 meters. A person has difficulty distinguishing objects located at a short distance from him. If measures are not taken, the patient will not be able to distinguish objects even at a distance of half a meter from himself. Remember that myopia can progress quickly. With this pathology, deformation of optical structures is observed: the retina, blood vessels and tissues. A person with moderate myopia is advised to wear contact lenses or glasses. In case of pathological changes in the structures of the optical apparatus that accompany myopia, laser correction or ophthalmological surgery is performed.
High (myopia 3rd degree)
This pathology is characterized by impaired blood supply to the visual apparatus, which greatly affects the retina. Also, with a high degree of myopia, the eyeball becomes deformed towards enlargement. A person distinguishes objects no further than his outstretched arm. At this stage of the pathology, only surgical intervention will help:
- scleroplasty;
- lasectomy;
- laser correction;
- excimer.
Excimer and laser correction are carried out if vision has dropped to 15 diopters. When vision loss exceeds 20 diopters, lens replacement is required. Scleroplasty is indicated to strengthen the corneal layer.
Treatment
The main methods of treating myopia are glasses, contact correction, and refractive surgery. Drug therapy, eye gymnastics, physiotherapy are methods that complement complex vision treatment.
Correction using optics
Optical correction of myopia includes the use of glasses and contact lenses. The purpose of optical correction is to move the focal point to the retina. For mild to moderate myopia, complete or incomplete spectacle correction is chosen.
Near glasses are selected depending on the state of accommodation. If the accommodative function is preserved, glasses for near vision are not used. When the “adaptive” power of the eyes decreases, glasses for near vision with lower optical power, with bifocal or progressive lenses, are selected. High myopia requires constant spectacle correction for distance and near.
Contact lenses have advantages over glasses. They are easy to use, create tight contact with the surface of the cornea, forming a single optical system with it. Contact lenses “unload” the eye muscles, taking on part of the optical function. For myopia, lenses not only support the muscular system of the eye, but also improve binocular vision and accommodation functions.
Medicines
Medicines used to relax accommodative muscles. This allows you to eliminate false myopia. The course of treatment should not exceed one week. When using them, paralysis of accommodation occurs, the pupil dilates, and near vision becomes blurred. Therefore, for the duration of use, you will have to stop driving a car, working on a machine, or a computer. It is advisable to take sick leave. Treatment is carried out strictly under the supervision of a doctor.
We recommend reading: Drops and vitamins for myopia
In the treatment of true myopia, drug therapy is an additional method. Vitamins are prescribed orally or intramuscularly, drugs to strengthen the vascular wall, improve blood supply to the eye, and increase immunity.
Physiotherapy
Physiotherapeutic methods are aimed at improving microcirculation of the eye, increasing the absorption of nutrients and rapid delivery of medications, relieving spasms of the eye muscles, and strengthening general immunity. Procedures applied:
- electrical stimulation through closed eyelids;
- laser massage;
- magnetic therapy;
- intranasal electrophoresis.
Neither method is primary. Application is strictly individual and is carried out under the supervision of a doctor in specialized medical institutions.
Surgical intervention
Corneal implants. Used to correct myopia from -3 to -8 diopters, for keratoconus. Plastic up to 0.45 mm thick and 6-8 mm in radius is implanted into the cornea. The surface of the cornea is smoothed, the optical power decreases. The implants can be easily removed if necessary.
Keratotomy is used for myopia with concomitant astigmatism. Radial incisions (3-12) are made surgically on the anterior surface of the cornea. As a result, elasticity decreases, pressure on the central region increases, and the cornea flattens.
The optical zone must remain intact. The disadvantage of treatment is a decrease in the strength of the cornea.
For myopia of more than -10 diopters, phakic lens implantation is used. Intraocular lenses are placed behind the iris, in the corner of the anterior chamber, or in the posterior chamber. The lens interacts with the cornea and lens, improving visual acuity and maintaining accommodation. However, there is a risk of developing secondary cataracts and increasing IOP.
For very high ametropia, it is possible to implant intraocular lenses with preliminary removal of the lens. In this case, it is impossible to maintain accommodation.
Laser correction
The advantages of laser vision correction are simplicity, speed, high efficiency and stable results. This is the most popular treatment method. The essence of the method is ablation (evaporation) of the upper layer of the cornea, changing the optical power. Suitable for myopia correction from -1 to -10 diopters.
PRK – photorefractive keratectomy. The PRK method removes the corneal stroma, changing the curvature. The operation requires the application of a contact lens or a removable bandage to the surgical wound area.
LASEK is a method of ablation of the cornea under the epithelial layer. LASIK is photoablation of the cornea under a lamellar cut. After ablation, the flap is placed in place.
Eye exercises
An important component of vision correction is regular eye exercises. The exercises are aimed at strengthening the eye muscles, training accommodative strength, improving blood circulation, and outflow of intraocular fluid. Exercises are performed standing or sitting with a straight back, the head looks straight, the body is relaxed, and unnecessary noise is excluded.
Basic techniques:
- blinking for 5-10 seconds, 5-10 approaches;
- pressing your fingers on the eyeballs through closed eyelids, 3-5 seconds, 5-7 approaches;
- holding your finger out in front of you, begin to slowly bring it closer to the bridge of your nose until the image begins to double, 5-6 times;
- eye movement alternately clockwise and counterclockwise;
- slowly shift your gaze from the ceiling to the floor for 1-2 minutes, 3-5 approaches;
- tracing the infinity sign with the eyes.
Folk remedies
Treatment of myopia at home is prohibited. You cannot use any drops yourself without a preliminary ophthalmological examination. Vision correction should be carried out under the supervision of a doctor. At home, you can take multivitamins in courses, eat fresh vegetables and fruits to improve vision and boost immunity. Perform eye exercises daily.
Structure and functions of the visual system
Knowledge about its structure will help to understand what happens in the visual system when myopia and farsightedness occur. Ophthalmologists distinguish two parts that make up the human eye: the retina and the refractive system.
The retina is a peripheral section consisting of a huge number of light-sensitive nerve cells. So, light particles, called photons, are reflected from objects around us, and then hit the retina. There, the generation of nerve impulses occurs, which are sent to the brain and projected into images. The refractive apparatus consists of a set of components responsible for focusing the image on the retina.
This complex includes:
- The cornea has a hemispherical shape and is endowed with a regular refractive power of approximately 40 diopters.
- The lens is a biconvex natural lens, fixed by ligaments and muscles in a special capsule. It is capable of changing its shape depending on the distance of the object in question, so its refractive power can vary from 19 to 33 diopters.
- The vitreous body is a colorless, jelly-like substance that fills the space between the retina and the lens and is responsible for maintaining the necessary shape of the eyeball. This substance has no refractive ability.
- Aqueous fluid is located in special parts of the visual system and surrounds the lens. This component is responsible for the nutritional function, transporting important substances to the cornea, natural lens and eye tissues. And due to the content of immunoglobulins in this liquid, it fights the appearance of viruses, harmful bacteria and microorganisms.
Possible complications
Long-term uncontrolled myopia leads to deterioration of eye health and prognosis of quality of life. The most serious complication is irreversible loss of vision. Possible complications include amblyopia - impaired visual acuity in one eye, even with myopia in both eyes. Divergent strabismus develops with maximum relaxation of accommodation when trying to view an object in the distance.
Cataract is secondary. It is a consequence of impaired nutrition and blood circulation in the structures of the eye. Retinal detachment is a frequent guest of advanced myopia.
Symptoms of myopia
Myopia is a disease that may not manifest itself for a long time. And only during medical examinations can an ophthalmologist see deviations from the norm. Most often, myopia occurs and develops during the school period, when the stress on the eyes becomes most intense. Therefore, it is necessary to take a closer look at the child’s behavior: perhaps he began to squint his eyes often, have difficulty seeing distant objects, inscriptions on the school board, or come closer to an object viewed in the distance. Myopia threatens to deteriorate not only distant vision, but also twilight vision. This means that a person has poor orientation in the evening, when it gets dark.
Symptoms of myopia can also manifest themselves in the form of recurring headaches, rapid and severe eye fatigue from outdoor games or driving. If a person wearing glasses or lenses experiences similar symptoms, he needs to immediately visit a specialist and undergo a comprehensive medical examination. It may be right to change your optics to another one. Myopia usually appears in childhood. Children, being in educational institutions, begin to have difficulty distinguishing distant objects and squint.
The best results of vision correction for myopia are achieved using lenses or glasses with a “minus” index. Sometimes you have to change lenses quite often, since such vision is easily impaired. It is important to note that glasses cannot prevent the development of myopia, but only help change the refraction of light rays. Frequently changing glasses from smaller to larger diopters indicates a significant progression of myopia and excessive stretching of the eyeball. At the same time, visual acuity is greatly reduced, the retina is so damaged that its complete detachment can occur. This situation threatens with very serious consequences, including complete loss of visual capabilities.
Prevention of myopia
To prevent the disease, various measures have been developed to prevent myopia. This disease develops mainly in children and adolescents, which means it is necessary to instill in them preventive skills from childhood. Prevention of myopia consists of the following: visual hygiene, performing gymnastic exercises for the eyes and undergoing general strengthening measures.
An important role is to undergo preventive examinations for the timely detection of myopia in the early stages, especially if the person belongs to a risk group. It is important to carry out clinical examination of patients with myopia, correct vision at the initial stage of the disease, and implement various preventive measures.
As a preventative measure, following these tips shows good results:
- You should strictly maintain a distance of 30 cm between your eyes and a book, monitor, phone, tablet and other devices. This distance reduces eye strain and avoids the occurrence of temporary or permanent myopia.
- Periodically give your eyes a chance to rest. If the eye is in a tense state for a long time, the risk of developing the disease increases significantly. Therefore, it is recommended to take a break every 40 minutes of work.
- It is very undesirable to read while lying on your back or side, or in moving transport (car, subway, train, etc.), since your eyes will strain trying to catch the text. The eyes are also strained when reading while lying down because one eye is further away from the text than the other.
- Correct posture is a prerequisite. The eyes see the object at the right angle if the person has a straight back.
- The lighting of the desktop should be optimal and comfortable so that the eyes do not strain too much. Sunlight is considered the best for human eyes. In the workplace, artificial lamps should be used to achieve similar light. If a person works in the evenings, then a desk lamp is a must.
- Ultraviolet rays have a detrimental effect on the retina of the eyes. It is imperative to ensure eye protection from them.
- Prevention of myopia is also compliance with proper nutrition. Constantly feeding the body with important vitamins and minerals ensures excellent eye function and less fatigue.
Myopia and farsightedness test
The duochrome test is an easy test that allows you to examine your vision and determine whether there are deviations from the norm in the direction of myopia or farsightedness. Such a home test is only indicative and subjective in nature, and therefore cannot replace a real examination by an ophthalmologist. The test is designed for timely assessment of visual defects.
How to conduct the test yourself?
- You must move one meter away from the computer monitor.
- You need to cover one eye lightly, without pressing hard on the eyelid, with your palm, and look at the picture with the other.
- Then change eyes.
- The test must be performed with contact lenses or glasses if the person already uses them.
Test conclusions:
- If vision is normal, then a person sees signs equally clearly with both eyes.
- If farsightedness is suspected, a person sees the signs clearer and darker on a green background.
- If there is a suspicion or tendency to myopia, a person sees signs better on a red background.
- Be that as it may, you should definitely undergo examination by a specialist.
Difference between farsightedness and nearsightedness
The main difference between farsightedness and nearsightedness is the location of the center of the picture. With farsightedness, light is concentrated behind the shell of the eye, and therefore images are transmitted to a person in a fuzzy, blurred form.
Light, in people with farsightedness, is located behind the retina for two main reasons:
1.
The size of the farsighted eye is much smaller than normal. This cause of farsightedness (hypermetropia) is more common than others. Even if the rays of light are refracted correctly, it still happens behind the retina.
2.
The eyes of a person suffering from farsightedness do not refract light as strongly as the eyes of a healthy or even nearsighted person. But this reason is quite rare. For example, a healthy eye refracts rays with a power of 42-45 diopters, while a far-sighted eye refracts rays with a power of 38-42 diopters.