Form vision and visual acuity
In clinical practice, vision is assessed using visual acuity and macular function tests, and this should be part of any complete medical examination, regardless of whether there are any relevant complaints. The Snellen chart (1862) is placed at a distance of 6 m from the patient. The Sivtsev table, used to determine visual acuity in the USSR, is placed at a distance of 5 m from the patient.
The Snellen chart consists of letters of varying sizes. The distance at which each size is reduced by an angle of 5° is indicated on the side of the table. A patient with corrected refractive error should wear glasses during the examination. Normal vision is 20/20. If the patient can read letters only up to the 20/30 line, visual acuity is defined as 20/30. If the patient is not able to distinguish the largest letter E on the top line, he must be transplanted to the table, thus changing the distance. Visual acuity can be defined as 10/400 if the patient can distinguish this letter at a distance of 3 meters from the table.
Using the Snellen table (placed at a distance of 6 m from the patient) or the Sivtsev table (placed at a distance of 5 m from the patient), the visual acuity of a person is determined.
If the patient cannot read the 20/30 line, stenopeic vision should be examined. Through the stenopeic foramen, which transmits a narrow beam of light rays, a patient with secondary vision loss due to refractive error must read lines up to 20/20. If visual acuity does not improve, you should look for another reason for its decrease, for example, clouding of the ocular media, spots or damage to the optic nerve.
Visual acuity corrected with glasses or contact lenses only to 20/200 or less on both sides, as well as concentric narrowing of the visual fields up to 10° in the United States is officially considered blindness, such a patient must be registered with the Society of the Blind at the place of residence.
Twilight vision disorder
What is twilight vision impairment? This disease has been known to medicine since ancient times and was called hemeralopia. Doctors do not distinguish between its degrees (the disease is either present or not), but ophthalmologists are confident that twilight vision disorder significantly reduces the quality of life, which sometimes has fatal consequences.
Hemeralopia is also called night blindness. This visual disorder is caused by damage to the optic nerve and retina. Its characteristic features are manifested by a decrease in visual acuity in the dark. It has the following symptoms:
- narrowing of fields of vision and transformation of light adaptation;
- decreased vision with impaired areal orientation at night.
Sometimes these symptoms are accompanied by problems with contemplating blue and yellow colors.
Hemeralopia affects both men and women equally. But when women go through menopause and endocrine adjustments occur in their bodies, their risk of night blindness is slightly higher. Interestingly, the Australian aborigines have a natural heightened vigilance, especially at night. Scientists have found that these people have visual acuity up to 400%.
The peoples of the North also see better in the dark. This skill has been developed over centuries, because there are very few sunny days in the North. That is why their eyes adapted to such an environment “historically”. In winter, when daylight hours become too short, the problem of hemeralopia worsens.
Color vision
Often, visual impairment in humans is characterized by acquired defects in color perception. For example, in some cases of damage to the macula (due to intoxication or degenerative causes) or the optic nerve (multiple sclerosis, toxins, drugs, malnutrition, tobacco-alcohol amblyopia), patients do not distinguish between red and green colors, although they perceive white color normally.
Ishihara polychromatic tables are most often used to study color vision. Polychromatic Ishihara tables, which help identify visual defects in red and green colors, and Hardy-Rand-Ritler (GRR) figures, which help identify impaired perception of red and green, as well as blue and yellow colors. To work in some professions, a person requires fully preserved color vision. Hereditary blindness to red, green and other colors (color blindness) is also possible.
When the macula is damaged as a result of intoxication or degeneration, patients do not distinguish between red and green, but they perceive white color normally.
Monocular vision
Many people ask the question: “Monocular vision – what is it?” With this vision, moving objects and objects that appear in the field of vision of the looking person are captured mainly by only one eye.
In ordinary situations, people with normal vision use binocular vision, that is, they evaluate visual information with two eyes. Monocular vision is typically measured in angular terms.
It is known that birds have very extensive all-round vision. They see not only in front of them, but also to the sides, and even behind them. Birds have eyes on the sides. The quality of bird vision exceeds the acuity of human vision by four to five times.
The total field of vision in birds reaches more than 300° (the field of vision of each eye of a bird is 150-170°, which is 50° more than that of a human). Birds mainly use lateral (lateral) and monocular vision (this is normal for them). Its general field is localized at approximately 70°. But in owls, the eyes do not move at all, which is compensated by the agility of the neck (approximately 270°).
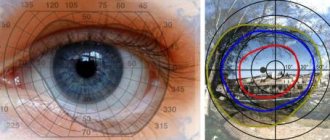
Light perception and visual field studies (perimetry)
A person's light perception is assessed using visual field testing. The procedure for studying visual fields is called perimetry. Changes in visual fields indicate damage to the portion of the visual tract from the retina (along the optic nerve) to the visual cortex. The most convenient method for studying visual fields is the kinetic perimetry method (Goldmann hemispheric perimeter). It consists of moving an object in the fields of view and establishing points of equal sensitivity in two fields. During perimetry, the patient gives a signal when he sees an object, indicates when it disappears and when it then reappears. In this way, a diagram of the patient's visual fields can be drawn up with a precise indication of the defects from the periphery to the point of central fixation. You can also compare the peripheral visual fields of the patient and the doctor.
Examination of the visual fields (perimetry) reveals its defects and their location during the diagnostic perimetry procedure.
Visual fields are considered normal if a person sees an object during visual field diagnostics during perimetry:
- 90° - with perimetry from the side of the temple
- 50° - with perimetry from the side of the nose
- 50° - with perimetry upward
- 65° - with perimetry downwards
The listed visual impairments in patients can occur either individually or in combination. Such visual impairment in patients can occur as a result of changes in the refractive (refractive) properties of the transparent media of the eye, lesions of the retina, optic nerve or other parts of the brain with which they are connected.
What is eye refraction?
What do the terms “minus” and “plus” mean? These are standards for diopters - units in which the refraction of the eye is measured. Refraction is the location of the eye relative to the retina. There are three types of refraction:
- Hyperopia is the placement of the focus behind the retina, that is, farsightedness. Denoted by the word "plus".
- Emmetropia is vision without refractive errors when the focus is on the retina. In this case, the refraction is 0.
- Myopia - the focus is in front of the retina, which causes distortion of distance vision, blurred images or contours. Diopters are marked with the word “minus”.
What does a person see
Thanks to vision, we receive 90% of information about the world around us, so the eye is one of the most important sense organs. The eye can be called a complex optical device. Its main task is to “transmit” the correct image to the optic nerve.
Structure of the human eye
The cornea is the transparent membrane that covers the front of the eye. It lacks blood vessels and has great refractive power. Part of the optical system of the eye. The cornea borders the opaque outer layer of the eye, the sclera.
The anterior chamber of the eye is the space between the cornea and the iris. It is filled with intraocular fluid.
The iris is shaped like a circle with a hole inside (the pupil). The iris consists of muscles that, when contracted and relaxed, change the size of the pupil. It enters the choroid of the eye. The iris is responsible for the color of the eyes (if it is blue, it means there are few pigment cells, if it is brown, it means a lot). Performs the same function as the aperture in a camera, regulating the light flow.
The pupil is an opening in the iris. Its size usually depends on the light level. The more light, the smaller the pupil.
The lens is the “natural lens” of the eye. It is transparent, elastic - it can change its shape, almost instantly “focusing”, due to which a person sees well both near and far. Located in the capsule, held in place by the ciliary band. The lens, like the cornea, is part of the optical system of the eye. The transparency of the human eye lens is excellent, transmitting most light with wavelengths between 450 and 1400 nm. Light with a wavelength above 720 nm is not perceived. The lens of the human eye is almost colorless at birth, but becomes yellowish with age. This protects the retina from exposure to ultraviolet rays.
The vitreous is a gel-like transparent substance located in the back of the eye. The vitreous body maintains the shape of the eyeball and is involved in intraocular metabolism. Part of the optical system of the eye.
Retina - consists of photoreceptors (they are sensitive to light) and nerve cells. Receptor cells located in the retina are divided into two types: cones and rods. In these cells, which produce the enzyme rhodopsin, the energy of light (photons) is converted into electrical energy of the nervous tissue, i.e. photochemical reaction.
The sclera is the opaque outer layer of the eyeball that merges at the front of the eyeball into the transparent cornea. 6 extraocular muscles are attached to the sclera. It contains a small number of nerve endings and blood vessels.
The choroid - lines the posterior part of the sclera, adjacent to it is the retina, with which it is closely connected. The choroid is responsible for the blood supply to intraocular structures. In diseases of the retina, it is very often involved in the pathological process. There are no nerve endings in the choroid, so when it is diseased, there is no pain, which usually signals some kind of problem.
Optic Nerve - The optic nerve carries signals from nerve endings to the brain.[6]
A person is not born with an already developed organ of vision: in the first months of life, the formation of the brain and vision occurs, and by about 9 months they are able to almost instantly process incoming visual information. In order to see, light is needed. [3]
What is necessary for the development of normal binocular vision?
Binocularity begins to develop in children after two months after birth. In the first 6-8 weeks, the extraocular muscles cannot yet work in concert, so infants do not have stereoscopic vision. The baby should be able to clearly focus his eyes on an object at 3 months. If this does not happen, then parents should visit an ophthalmologist for an examination. The process of developing binocularity is completely completed by about 12-14 years.
For the proper development of binocular vision, the following conditions must be present:
- the same shape of the cornea in the left and right eyes;
- the difference in optical power between the eyes should not exceed 0.5 diopters, and visual acuity should be 0.3-0.4. It is these factors that make it possible to form a clear image on the retina;
- normal functioning of the extraocular muscles, ensuring good mobility of the eyeballs and coordination of movements. In old age, weakening muscle mobility is one of the reasons for the loss of binocular vision;
- absence of aniseikonia - difference in the size of both images;
- symmetry of the shape of the eyeballs;
- absence of visual pathologies.
Violation of any of the above conditions can affect the fact that binocular vision will be absent. In such a situation, other types of vision are present: monocular - the ability to see with only one eye; monocular alternating - the ability to see alternately with the left or right eye; simultaneous - a person sees with both eyes, but the picture is not combined into a single visual image.
Heterophoria
Ideal muscular balance in both eyes is called orthophoria . With orthophoria, in the case of separation of the eyes (for example, by covering one of them or placing a prism on it with the base up or down), the symmetrical position of both eyes and the vertical direction of the vertical meridians of the corneas are maintained. Orthophoria creates optimal conditions for binocular fusion of images of the object in question and facilitates visual work.
Much more often than orthophoria, heterophoria , in which there is unequal force of action of the extraocular muscles, caused by anatomical and nervous factors (features of the position of the eyeballs in the sockets, impulses to convergence and divergence, the relationship between accommodation and convergence, tone of the extraocular muscles, etc.) . Heterophoria, or hidden strabismus, is expressed in the deviation of one of the eyes during a period when a person does not fixate any object. Heterophoria is characterized by the presence of binocular vision and is detected only in cases where we intentionally or accidentally disrupt binocular fixation.
Depending on the direction of deviation of the eyes, heterophoria is divided into:
- exophoria – deviation towards the temple,
- esophoria - to the nose,
- hyperphoria - upward,
- hypophoria - downwards.
Methods for studying heterophoria are based on the principle of excluding one eye from the act of binocular vision.
Assessment of binocular vision in children
After the birth of the baby, parents should be attentive to his vision and pay attention to inconsistencies that arise during the development process. At three months, the baby should already be able to consistently focus his eyes on the toy in front of him. By this same age, infantile strabismus, with which all children are born, should improve. If it does not go away, then this is an obvious pathology and you should urgently visit an ophthalmologist. You should also pay attention to how the baby looks at pictures in books. If he lingers for a long time on one drawing and does not move it, this is also a reason to sound the alarm.
The lack of binocular vision in a child is usually fraught with two problems - strabismus or amblyopia (lazy eye syndrome). Strabismus most often develops before the age of three, which is why it is important to monitor it closely during this period.
Amblyopia is a visual impairment when one eye is not involved in the process of perceiving a picture, in other words, the child has monocular vision. Moreover, strabismus can cause amblyopia, and vice versa. This pathology is dangerous because if not treated in a timely manner, the functions of the diseased eye can completely atrophy.
Why is binocular vision so important?
Without binocularity, we would experience great difficulties in life. This nature of vision allows one to orientate well in space, assessing the distance to objects and between them (without this ability a person would not be able to work in many areas). It also promotes good peripheral vision and allows us to see the world in 3D projection - we can evaluate the size of an object, its shape, and relief. In addition, if vision is binocular, this contributes to the sharpness of vision and the brightness of the picture.
The lack of stereoscopic vision limits a person’s ability to engage in many activities in which an accurate assessment of the distance to an object and its size are important. In many professions this aspect is key. What kind of job can a person with impaired binocularity not work in?
- A medical worker of a certain direction: nurse, dentist, surgeon. Imagine that a surgeon, during an operation with a sharp scalpel, cannot estimate the distance to the patient’s organ and makes careless movements? A nurse without binocularity simply will not be able to give an injection into a vein.
- Driver of various types of ground transport, pilot.
- An athlete. It is simply impossible to engage in some sports in the absence of stereoscopic vision: in football, hockey, tennis and other sports, it is necessary to estimate the distance to a game object (ball, puck), player, goal; distance assessment occurs literally every second. But, for example, you can practice chess or swimming.
- Other professions include videographer, photographer, hunter and others.