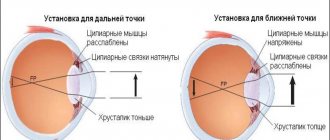
Translated from Latin, “accommodation” means “adjustment.” This term entered ophthalmology as a designation for the ability of the eye to equally clearly perceive objects located in the field of view at different distances. The coordinated operation of this mechanism is due to the functional interaction of three elements of the eye: the ciliary muscle, the ciliary ligament and the lens.
In a calm state, the eye is tuned to distance vision. In this case, accommodation is provided by muscles that are in a relaxed state. When you shift your gaze to nearby objects, the ciliary muscle (ciliary) contracts with simultaneous relaxation of the zonules of cinnamon. The consequence of this is an increase in the curvature of the surface of the lens - the elastic transparent element of the eye, responsible for focusing light rays on the retina. The projection of a clear image onto its photosensitive surface is ensured by an increase in the optical power of the lens to 12-13 diopters.
When there is no need for accommodation on nearby objects, the ciliary muscle relaxes, the refractive power weakens, and the eye focuses on infinity. Distance accommodation is also called disaccommodation.
The accommodative function is closely related to the condition of the lens. Clear vision requires its ideal transparency and good elasticity. The lens is most elastic in childhood; With age, mechanical elasticity is gradually lost, which is responsible for the decrease in the acuity of “near vision” in many people after 40-45 years. In this case, age-related farsightedness (presbyopia) is diagnosed. By the age of 60-70 years, the ability to accommodate may be completely lost.
Accommodation in twilight conditions is carried out somewhat differently. In the dark the eye sees only at short distances; disaccommodation “does not work”, the visual system strives to make maximum use of the available level of illumination and focuses on nearby objects. Under such conditions, in a person with a refractive error, hyperopia (farsightedness) decreases by 2.0 diopters, and myopia increases to the same extent. Normal vision behaves like myopia.
Reasons for the development of false myopia
Under optimal lighting conditions, the image on the retina becomes out of focus. This provides an incentive to activate the mechanisms of accommodation. When the projection of rays from objects viewed nearby is focused blurry on the retina, the brain perceives this as a need for correction and sends impulses to the structures responsible for accommodation. This command travels along the oculomotor nerve to the ciliary muscle, causing it to contract. Under the influence of muscle force in combination with relaxation of the zonules of Zinn, the curvature of the lens changes. This adjustment stops at the moment when the image is clearly focused on the retina. Shifting your gaze into the distance again relaxes the ciliary muscle, since focusing in the plane of the retina occurs without its tension, as a result of which the curvature of the surface of the lens decreases and it becomes flatter.
Accommodation spasm can develop under the influence of the following factors:
- exceeding the permissible visual load (reading, watching TV, working at a monitor, sewing and other activities that require constant visual concentration);
- habitually insufficient illumination of the workplace;
- unhealthy daily routine, certain imbalances in work and rest schedules;
- the distance from the work surface to the eyes is too close (often this is allowed by insufficiently attentive parents when the furniture, i.e. the work table and chair, does not correspond to the child’s height);
- bad habit of placing the book too close to the eyes when reading;
- postural disorders associated with weakness of the cervical spine and back muscles;
- blood supply problems in the cervical spine;
- general lack of physical activity.
↑ Structure of the ciliary muscle
The question of the mechanism of accommodation is the subject of a large number of scientific studies and theories.
When an object approaches a constant light-refracting optical system, the image it creates will move away from it and, conversely, when the object moves away from the eye, the image will approach the retina (Fig. 1).
In the accommodation of the human eye, according to Helmholtz's theory, there are two parts - active and passive. The active part is carried out by the ciliary, or accommodative, muscle, the passive part is carried out by the ligament of Zinn and the lens.
The ciliary muscle, located in the ciliary body, belongs to the smooth muscles and consists of three types of muscle fibers with at least double innervation. In cross section, it has the shape of a triangle, becoming thinner towards the flat part of the ciliary body. The presence of the muscle gives the ciliary body its characteristic (in cross-section) triangular shape.
The muscle fiber bundles are located in three directions: meridional, circular (or equatorial) and radial.
The meridional fibers (Brücke muscle) are located under the sclera itself, parallel to it and form
the outer part of the ciliary muscle. Originating from the inner layers of the choroid and the border plate of the vitreous, they stretch to the limbus, where they attach to the scleral spur and partly to the trabeculae. Circular fibers (Müller's muscle) are located in the anterior internal part of the ciliary body in the form of separate ring-shaped muscle bundles. From the scleral spur, radial fibers (Ivanov's muscle) diverge in a fan-shaped manner to the pars plana and processes of the ciliary body.
Accommodation indicators
The ability of the eye to accommodate is measured in diopters or linear values.
- Functional rest of accommodation - disaccommodation - focusing to infinity in the absence of an accommodative stimulus in the visible zone. The accommodation area is the distance along the main optical axis of the eye between the extreme points of clear vision (near and far).
- The volume of accommodation is the range of changes in refractive index, expressed in diopters, when focusing on the nearest and most distant points of clear vision.
- Accommodation stock (reserve) is the unused part of the accommodation capabilities at a certain point in the visual field, located at a given distance.
In the process of ophthalmological diagnostics, absolute and relative indicators of accommodation can be determined. Examination of each eye separately gives absolute values. Diagnosis of both eyes, performed with a certain convergence (reduction) of the visual axes, makes it possible to determine relative indicators.
The functions of accommodation are inextricably linked with convergence. At the same angle of convergence of visual lines, the degree of accommodation in people with different indicators of visual acuity is not the same. For example, uncorrected farsightedness in children (hyperopia) can lead to accommodative convergent strabismus.
Violation of accommodation can manifest itself in the following forms:
- spasm of accommodation;
- paralysis and paresis of accommodation;
- accommodative asthenopia;
- presbyopia (age-related decrease in accommodation).
Children and young people are most susceptible to accommodation spasms. This spasm is caused by functional disorders in the ciliary body, which leads to weakened vision both near and far. The spasmodic ciliary muscle remains in a state of accommodating tension even in situations where its relaxation is required. The development of accommodation spasm is especially facilitated by educational overload; This is why this type of disorder occurs predominantly among schoolchildren and students. According to the results of statistical studies, every sixth student has accommodation disorders caused by muscle spasms.
Paralysis and paresis (partial paralysis) of accommodation can also be a consequence of injuries and the action of toxins. In addition, this type of accommodative disturbances is often provoked by neurogenic factors. In this case, the degree of myopia may not change or increase insignificantly, but the acuity of normal and presbyopic vision decreases at close distances. In any case, paralysis and paresis lead to a reduction in accommodative reserves and a decrease in the overall volume of accommodative capabilities.
Accommodative asthenopia often results from incorrect selection of glasses or lenses for farsightedness and astigmatism. Inadequate optical correction causes rapid visual fatigue, redness of the eyes, itching in the eyelids, dry sclera and an increasing sensation of foreign particles in the eye (chronic blepharoconjunctivitis). Visual discomfort can cause headaches, nausea and even vomiting, which is associated with excessive tension of the eye muscles with limited accommodation reserves.
Age-related accommodation disorders (presbyopia) develop due to gradual involution (reverse development, age-related degradation) of the lens under the influence of external factors and a gradual decrease in the rate of metabolic processes in old age. Over time, the lens loses elasticity, thickens, and becomes less transparent; the eye muscles are no longer able to give it the required curvature and provide sufficient optical refractive power with such changes.
Habitually excessive tension of accommodation (PINA)
This is a chronic overstrain of the ciliary muscle, leading to the appearance of myopic refraction (false myopia - pseudomyopia).
The following features are noteworthy:
- school age, adolescence,
- complaints of decreased distance vision,
- develops gradually
- the appearance is associated with an increase / intensification of visual load.
Many clinical and experimental studies have proven the connection between accommodation disorders and childhood myopia, as well as the progression of myopia. PINA is inextricably linked with myopia, so it makes sense to remember what factors influence the appearance and progression of myopia.
The chain is built as follows: heredity, trauma to the cervical spine, unfavorable environmental conditions, excessive visual load -> pseudomyopia, PINA -> true myopia, PINA -> progression of myopia -> complications of myopia.
PINA is most often caused by prolonged, abnormal visual load at the wrong distance.
Myopia appears (but this is false myopia), which completely corrects vision to 1.0 (100%)
The mistake in this case would be to immediately prescribe glasses. After a course of treatment with drugs that relax the ciliary muscle, and a visual load determined by the doctor, glasses may not be needed. There are cases when, after a course of treatment, false myopia turns into farsightedness.
The sooner a child starts using tablet computers and similar electronic devices, the sooner and more likely he will develop PINA, which turns into myopia.
Symptoms of spasm of accommodation
Signs of false myopia:
- working at close range causes rapid fatigue;
- the eyelids and sclera turn red during visual stress, burning and itching are felt;
- near visual acuity decreases, distant objects also appear blurry or double;
- performance and academic performance decreases;
- headaches occur systematically, especially after visual strain.
Often, the changes that have begun last and progress for years. The person himself perceives them as a natural process of age-related adjustment, although the real reason may lie in physiological visual disturbances that are quite amenable to correction.
Classification of disorders
There are several types of disorders of the accommodative apparatus:
- Accommodation spasm is a sharply increased accommodation tone. At the same time, the person suddenly notices that he has begun to see the image in the distance blurry. A common disorder of ocular accommodation in children.
- PINA (habitually excessive tension of accommodation) – long-lasting tone. Distance vision deteriorates, but corrected visual acuity does not decrease.
- Weakness of accommodation is a weakened ability to move the gaze from one object to another.
- Accommodative asthenopathy is a disorder of refraction and accommodation, in which the eyes quickly tire. Occurs due to uncorrected myopia, hyperopia, and astigmatism.
- Presbyopia is an age-related accommodation disorder that develops in people over 40 years of age. Characterized by clear distance vision with deteriorating near vision.
- Paresis or paralysis of accommodation is a disorder caused by paresis (incomplete weakening) or paralysis (complete lack of function) of the ciliary muscles. With this disorder, a person always sees blurry.
- Violation of accommodation after vision correction operations. The most common difficulty is translating one's gaze to a close distance.
Spasm, paresis and paralysis can be caused by insufficient blood flow, cancer, head injuries, infection, and neurological diseases. These disorders are the most dangerous to health.
Weakness of accommodation and PINA lead to deterioration of vision, regular headaches and eye pain, redness, and irritation of the eye.
Prevention and treatment of accommodation spasm
False myopia in the absence of adequate treatment and correction leads to the development of true organic disorders. Constant spasm prevents normal vasculature (blood supply) of the ciliary muscle, as a result of which it weakens. This is the mechanism of development, in particular, of chorioretinal dystrophy with functional accommodative weakness. Currently, it is the spasm of accommodation that is considered as the main cause of childhood myopia (first false, and then true myopia).
Our ophthalmological center has everything necessary to identify and effectively eliminate false myopia in both children and adults. The treatment uses not only eye drops and eye exercises, which the patient can do himself at home, but effective hardware techniques that can be used to relieve accommodation spasms in several sessions: quickly and harmlessly!
Treatment of accommodation spasm consists, first of all, in a system of visual exercises and training on special computer simulators. Mydriatic drops (dilating the pupil), laser treatment, magnetic and electrical stimulation are also used. Good results are achieved by massage of the cervical-collar area, the course of which is recommended twice a year. Vitamins and a varied diet are prescribed as general strengthening therapy. For students, it is extremely important to normalize the work and rest schedule, which necessarily includes periods of physical activity.
Drops to relieve spasm of accommodation
Eye drops that dilate the pupil (Irifrin, Tropicamide, Midriacil, etc.) are usually used at night. This makes it possible to provide a relaxing effect on the accommodative muscle that is sufficient in strength and time, while maintaining the patient’s ability to have good vision during the day.
In addition, so-called “vascular and vitamin” drops - Taufon, Emoxipin, etc. - can be prescribed in complex therapy. They improve microcirculation in the tissues of the eyeball and help improve visual functions.
Exercises for false myopia
Gymnastics for the eyes, aimed at training accommodation, primarily involves focusing the gaze on equidistant objects.
The most popular exercise is the so-called “mark on glass”, which consists of the following:
A mark (about 5 mm in size) is attached to the window glass; it can be a small sticker or a spot drawn with a marker or any other means at hand.
After this, you need to move 0.5 meters away from the glass and find a distant object (tree, building, etc.) on the street (behind this mark), then you need to alternately look from the indicated distant landmark to the mark.
The exercise is performed 10-20 times per “approach to the window.” During the day you need to repeat the gymnastics 3-5 times. This allows you to develop a spasmodic accommodative muscle of the eye.
Timely measures taken to prevent spasm of accommodation are effective prevention of more serious disorders accompanying true myopia.
Accommodative asthenopia
This is a symptom complex that includes discomfort, fatigue during prolonged work, and decreased vision at distance and near. Patients report pain.
During the examination, there may be slight refractive errors (myopia, hypermetropia), which are either not corrected at all or incorrectly corrected.
It is necessary to use adequate optical correction, stimulate the ciliary muscle, and use adrenergic agonists.
If you feel that your vision has deteriorated - this is interfering with work, reading, etc., you should consult an ophthalmologist to determine the cause. The doctor can make the right decision based on the examination and examination: what measures to take, whether to prescribe treatment or choose glasses for temporary or permanent wear.