Blood vessels create dense plexuses in the ciliary body, directly feeding the ciliary body, as well as the iris. The smallest capillaries in the ciliary processes continuously form intraocular fluid in the volume necessary for the functioning of the eye, through filtration from the bloodstream. Intraocular fluid creates constant intraocular pressure, which ensures all the basic functions of the organ of vision. At the same time, the ciliary body, attached to the protrusion of the sclera, serves as a support for the next element of the choroid - the iris.
Content:
- 1 Structure of the ciliary muscle
- 2 Accommodation mechanism
- 3 Innervation of the act of accommodation
- 4 Accommodation study
- 5 Determination of accommodation reserves and their stability
- 6 Study of convergence, its reserves and sustainability
- 7 Signs of accommodation spasms
- 8 Causes of accommodation spasms
- 9 Types of accommodation spasms 9.1 Artificial accommodation spasm
- 9.2 Physiological spasm of accommodation
- 9.3 Pathological spasms of accommodation
Description
Functions of the ocular structure
The main purpose of the ciliary muscles is to ensure accommodation processes. The functions of this organ are distributed among the fibers in its composition. Brücke's muscles ensure the forward movement of the ciliary muscle and promote focusing on distant objects (disaccommodation). The radial muscles are also involved in long-distance vision.
Disaccommodation plays an important role when moving in space and turning the head. When performing such actions, it serves to project a clear image on the retina.
The Müller muscle provides the opposite phenomenon of disaccommodation - accommodation. The essence of this process is equally good visualization of near and distant objects.
↑ Structure of the ciliary muscle
The question of the mechanism of accommodation is the subject of a large number of scientific studies and theories.
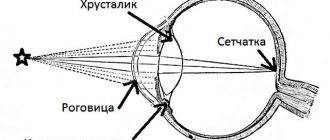
When an object approaches a constant light-refracting optical system, the image it creates will move away from it and, conversely, when the object moves away from the eye, the image will approach the retina (Fig. 1).
In the accommodation of the human eye, according to Helmholtz's theory, there are two parts - active and passive. The active part is carried out by the ciliary, or accommodative, muscle, the passive part is carried out by the ligament of Zinn and the lens.
The ciliary muscle, located in the ciliary body, belongs to the smooth muscles and consists of three types of muscle fibers with at least double innervation. In cross section, it has the shape of a triangle, becoming thinner towards the flat part of the ciliary body. The presence of the muscle gives the ciliary body its characteristic (in cross-section) triangular shape.
The muscle fiber bundles are located in three directions: meridional, circular (or equatorial) and radial.
The meridional fibers (Brücke muscle) are located under the sclera itself, parallel to it and form
the outer part of the ciliary muscle. Originating from the inner layers of the choroid and the border plate of the vitreous, they stretch to the limbus, where they attach to the scleral spur and partly to the trabeculae. Circular fibers (Müller's muscle) are located in the anterior internal part of the ciliary body in the form of separate ring-shaped muscle bundles. From the scleral spur, radial fibers (Ivanov's muscle) diverge in a fan-shaped manner to the pars plana and processes of the ciliary body.
Ciliary muscle: structure, functions, symptoms and treatment
The human eye adapts and sees objects equally clearly that are at different distances from a person. This process is ensured by the ciliary muscle, which is responsible for the focus of the organ of vision.
According to Hermann Helmholtz, the anatomical structure in question, at the moment of tension, increases the curvature of the eye lens - the organ of vision focuses the image of nearby objects on the retina. When the muscle relaxes, the eye is able to focus the image of distant objects.
↑ Accommodation mechanism
Helmholtz (1855) believed that during the rest of the ciliary muscle, the ligament of Zinn is “tight. It is connected on one side with the ciliary body, and on the other with the lens bag and exerts some pressure on the latter. As a result of this action on the lens capsule, the ligament of Zinn does not allow it to take on a more convex shape, which it could have due to the elasticity of its fibers.
The accommodative muscle, during its contraction (the immobile beginning of the muscle at the skeleton of the angle of the anterior chamber of the eye), pulls the posterior part of the ciliary body and the anterior part of the choroid anteriorly. At the same time, the fibers of the zinc ligament relax, the forces tensing the lens capsule decrease, and due to elasticity it becomes more convex.
Helmholtz noted the following changes in the human eye during accommodation:
- constriction of the pupil during accommodation for near, dilation during disaccommodation (found by Scheiner back in 1619).
- Moving forward (into the anterior chamber) the center of the anterior surface of the lens and the pupillary edge of the iris.
- The surfaces of the lens become more convex during accommodation (the anterior one is larger than the posterior one) and less convex during disaccommodation. This was noted by Scheiner (1619) and Descartes (1619) (cited by M?tze, 1956). The first accurate studies of this phenomenon were given by Langenbeck (1849) and Kramer (1854; cited by Mütze) and independently by Helmholtz (1655). The thickness of the lens increases with accommodation by 0.4
mm (from
3.6
to
4.0
mm). - During accommodation, the peripheral belt of the iris moves slightly posteriorly, so that a depression of the anterior chamber is formed (especially in children). Gulstrand clearly observed this phenomenon using a corneal microscope, as well as the forward movement of the central part of the anterior surface of the lens. In addition, Hess (1903, 1909) observed that the lens moves downward by 0.25-0.3
mm during accommodation (Hess's phenomenon) and that with small movements of the eye there is a tremor of the lens.
These observations provide very significant support for Helmholtz's theory, as they confirm the relaxation of the fibers of the ligament of Zinn during accommodation.
↑ Innervation of the act of accommodation
Many studies have been devoted to the question of the essence of the accommodation process. For theory and clinical practice, questions about the innervation of the accommodative process and the essence of the “rest” state of the accommodative muscle are of paramount importance.
Back in 1866, Trautveter found that when the oculomotor nerve is irritated, the Purkinje-Sanson figures decrease, which indicates a decrease in the radius of curvature of the lens surfaces. This confirmed the idea that accommodation is carried out using parasympathetic innervation (as part of the oculomotor nerve).
This view was shaken after the publication of the results of the experiments of Mogakh and Doyon (1891), according to which a decrease in the Purkinje-Sanson images was observed during irritation and an increase when the cervical sympathetic trunk was cut. This observation showed that there is a double innervation of accommodation: the oculomotor nerve for close distances, the sympathetic nerve for distances.
Both opponents and defenders of this view appeared in the literature. Thus, Hess and Heine (1898) were unable to confirm with their experiments the participation of the sympathetic nerve in the innervation of accommodation. Lokshin (1938) on 20
animals after excision of part of the cervical sympathetic trunk on one side could not skiascopially find changes in the refraction of the eye.
However, the hypothesis of double innervation of the act of accommodation has found many supporters and over time their number is increasing. Poos (1928) used ephedrine, cocaine, and adrenaline in the form of drops or subconjunct injections, which irritate the sympathetic nerve. In all his experiments, under the influence of drugs irritating the sympathetic nerve, a mild paresis of accommodation was observed, which proved the presence of sympathetic innervation.
Cogan (1937) skiascoped the eyes of animals before and after stimulation of the sympathetic nerve. He also received evidence of the presence of sympathetic innervation, because refraction when irritated by the sympathetic nerve changed towards hypermetropia. Castelli (1935) 29
a person found accommodation paresis from
1.0
to
3.0
D after using adrenaline. I. S. Shimkhovich (1941), T. K. Dzharakyan (1946) obtained a clear distance from the nearest point of clear vision under the influence of subconjunctival injections of adrenaline.
S.I. Polner (1946) in the clinic led by prof. E. Zh. Tron, studied accommodation using the ergograph of A. V. Lebedinsky and N. I. Zimkin (1936) before and after the action on the eye 5%
cocaine solution drop by drop
3
times a day and adrenaline (
1:1000
) in the form of subconjunctival injections.
These observations allowed him to identify the occurrence of accommodation paresis with an average of about 2.0
D and thereby confirm the participation of the sympathetic nerve in the innervation of accommodation.
A. V. Lebedinsky (1948), summing up numerous studies of this issue, came to the conclusion that there is an undoubted presence of double innervation of the act of accommodation. Somewhat later, Meesmann (1952) and Monje (1952) came to the same conclusion. Both authors confirmed the opinion expressed by A.V. Lebedinsky (1948) that adrenaline can limit the experimental tension of accommodation.
They write that irritation of the parasympathetic nerve causes contraction of the ciliary muscle, while the use of sympathomimetic substances weakens the muscle. These authors propose to consider the relaxation of the accommodative muscle not as passive, as it was previously considered, but as an active process. By this they revise the concept of rest of the accommodative muscle, believing that its state when installed at a distance depends on the tone of the autonomic nervous system, taking into account the state of the antagonists - the sympathetic and parasympathetic nerves.
Thus, the generally accepted idea that the accommodative muscle is at rest at distance should indeed be reconsidered. Recognition of the presence of antagonistic innervation of the ciliary muscle entails the recognition that when one part of it is relaxed (for example, the circular one), the tone of the second increases.
Even V.P. Odintsov (1938) wrote that, although accommodation is understood as the ability of the eye to enhance refraction, “strictly speaking, the reverse process should also be included in the phenomena of accommodation - weakening of refraction, necessary for transferring vision from closer to more distant objects.” .
In this regard, the work of the Baku Ophthalmological School, led by prof. U. X. Musabeyli. The increase in refraction (towards myopia) obtained by U. X. Musabeyli and K. A. Adigezalova-Polchaeva (1958) when the eye is exposed to agents that block the sympathetic nervous system is another proof of the correctness of the issue of antagonistic autonomic innervation of the ciliary muscle. U. X. Musabeyli recommends that in order to determine the true refraction, in addition to atropine, which paralyzes the annular part of the ciliary muscle (Müller’s muscle), also use adrenaline, which stimulates accommodation into the distance.
A very quick and effective way to relax your eyes
I don't know if all programmers are comprehensively curious people, but I always try to gain fundamental knowledge in all areas that can be practically useful. At the time when this idea came to my mind, I was studying anatomy and physiology in the magazines “Human Body. Outside and Inside”, but at work I was engaged in stereo-vario photographs (for those who don’t know, there were such Soviet calendars with a ribbed surface, where the picture either seemed three-dimensional or changed). So, one evening I came up with a wonderful idea, which I have been using for the past 4 years to maintain my vision.
I promise that you will feel the effect immediately!
Causes of visual impairment
There are 2 theories why a person’s vision deteriorates. In my opinion and experience, both of them occur.
Lens of the eye and ciliary muscles
First, let's take a look at why vision deteriorates: Myopia - corrected with a biconcave (reducing) lens.
Farsightedness is corrected using magnifying lenses.
Briefly about the reasons: loss of elasticity of the lens, spasm or “insufficiency” of the ciliary muscle - the muscle that changes the curvature of the lens.
Supporting muscles of the eye: lateral, medial and others
The photo shows the right eye
I will not describe in detail how and which eye muscles work - this can be easily understood by looking at the picture. I want to say only one thing: due to the uneven load on the muscles, some of them spasm, and either change the shape of the eyeball (and then, even with normal functioning of the lens and ciliary muscles, the same picture is obtained as in the images above), or they simply “lead the eye to the side” - when you look at the monitor screen, both of your eyes look at one closely located point, and therefore only the muscle (medial) works that turns/squints the eye, so to speak, closer to the bridge of the nose. When you look into the distance, both eyes look exactly straight. So, when you try to look into the distance after working at the computer for a long time, your eyes cannot look exactly straight due to a spasm of the medial muscle.
The method itself
I don’t know, maybe someone did something similar before me, but this is my idea, not seen anywhere. It looks simple: a plate with pairs of balls, with a number written on each ball.
How to use
Download and print the sign. There are 3 files in the archive. One table is immediately ready for printing (table_done.doc), the other (table.doc) contains a macro, by changing the parameters of which you can change the appearance of the table to suit specific needs (more details below), and the third (table_done.pdf) contains a pdf (very convenient use on a tablet). Print it out and hang the chart on the wall at eye level. Stand at a distance of about 30 cm from it and try to combine pairs of balls into one ball. In other words, each eye should look at a separate ball. Principle
. As soon as you managed to combine the top pair into one ball, go lower. So try to go as low as possible. With each new step down, you relax the muscles of the lens, making the image blurred as if “Gaussian” (to achieve this effect, look as if through a sheet into the distance), but not disconnected.
In this way, go up and down several times. Lately I've been using this tablet on my tablet - it's very convenient and always at hand. The only thing I do is turn the screen brightness down to minimum.
Some clarifications and notes
There is a well-known exercise of changing the focus of vision where you look at a point on the window, and then look at a point somewhere in the distance. The principle here is this, BUT! If you lower yourself to the lowest pair of balls, your eyes will literally move apart, relaxing the medial muscle and training the lateral muscle. In addition, due to this same force relaxation, the ciliary muscle of the lens also reflexively relaxes.
About the macro and its parameters. I assumed that if with each new step the balls increased or decreased, then this would be more effective for nearsighted or farsighted people, but it was not possible to test my hypothesis - there were no people willing to practice regularly. Try it! It may be possible to correct damaged vision. It definitely won’t get worse (tested on myself for 3 years - I’ve never worn glasses, my eyesight is excellent, I sit at the computer for hours).
And finally, additionally, rapid blinking for a minute and circular eye movements will also be useful. All!
UPD1: Due to the fact that it turns out there is also “cross-viewing”. The picture clearly illustrates. In order to understand how you look, you need to combine any pair of balls into one and close your left eye. If you are looking at the right ball with your right hand, then you are doing everything correctly, if you are looking at the left one, then your “technique” is wrong! The right eye should look at the right ball, the left eye at the left.
UPD2: People with congenital myopia are better off not overdoing it. Try, but don't overexert yourself. Congenital myopia or farsightedness is either a curved shape of the eyeball initially, or something with the lens (shape, elasticity). If congenital poor vision has worsened over the years, it could be partly due to muscle spasm, then this technique may help somewhat.
UPD3: Re-uploaded the archive into zip and transliterated the file names.
UPD4: Application available on Android.
Author: Timur First published in Geektimes magazine, 04/14/2012
↑ Study of accommodation
The study of accommodation must be carried out in the form of determining its volume using the formula: A = (1/p)-(1/a)
, where
a
is further,
p
is the closest point of clear vision. Since a depends on the static refraction of the eye, the study comes down to determining the nearest point of clear vision using a conventional accommodometer.
More indicative for studying the influence of visual work on accommodation is the study of its stability, the study of which began in 1914. Lancaster and Williams (cited by N.I. Zimkin, 1937) found that the closest point of clear vision during long-term fixation of the test through 20—40
minutes begins to move away. Howe (1935) and Berens (1932) applied the ergographic principle for this purpose. The ergographic method, developed by A. M. Zimkina, N. I, Zimkin and A. V. Lebedinsky (1932), consists of continuously recording on a kymograph the positions of the nearest point of clear vision by maximally approaching and slightly moving away the test object (Fig. 2) .
Under 1
By the 1st closest point of clear vision on the ergograph, these authors understood the position of the Landolt optotype in front of the eye, at which the gap in the optotype ceased to be visible, by the
2nd
- the position corresponding to the moment the gap appeared when the optotype was moved away.
When the optotype is reapproached, the accommodation voltage again reaches its maximum value. The difference between the position of the 1st
and
2nd
points in young people is
2-4
cm, in older people it can reach
10-20
cm (Fig. 3).
With a stable nature of accommodation, the ergogram remains horizontal, i.e., the distance of the nearest point of clear vision from the eye does not change.
If stability is insufficient (Fig. 4), they change as the distance between 1
1st and
2nd
points of clear vision, and their distance from the eye - the oscillation curve becomes wider and acquires an ascending character.
Our clinic uses a simplified method for determining the stability of accommodation using a conventional accomodometer.
The examiner marks on the scale of this device the moment the test object disappears (1
-th point) and the moment of its appearance when moving away from the eye (
2nd
point). With the difference in readings for these points and their distance from the eye, a curve of accommodation stability is constructed. This technique is quite suitable for practical purposes; easily applicable in any conditions; limited to the use of such a simple device as an accomodometer; allows you to do without a recording ergograph.
N.I. Pilman in the book “Practical Issues of Pediatric Ophthalmology” (1967) writes that “eye ergographs are still of little use for everyday work. For practical purposes, it is enough to determine the reserve of accommodation and convergence and their stability using the method of A. I. Dashevsky.”
↑ Determination of accommodation reserves and their stability
To rationally characterize the state of accommodation and convergence and their stability, the reserves of these functions should be determined separately. We introduced this rule in 1940 and consists of studying accommodation reserves when turning off convergence and vice versa.
In front of the eye (refractive errors are completely corrected, the second eye is covered with a white shield) a concave glass is placed with a force of 0,5—1,00
. The subject, transformed by this into a slight hypermetrope, experiences some difficulty in reading the last line on the table to determine visual acuity, but now reflexively, through the appropriate strain of accommodation, strengthens his refraction and thereby overcomes the effect of a negative glass placed in front of the eye.
Since the eye-plus-glass system again becomes emmetropic, his visual acuity again reaches 1,0
within a few seconds.
This “load” continues by adding 0.5-1.0
D each time until the maximum number of diopters that the eye can overcome with the help of its accommodation is reached.
This number of diopters does not always correspond to the age-related volume of accommodation in a given person; in healthy eyes it can be equal to 2/3
to
3/4
of this volume.
Once the accommodation reserve (expressed in diopters) has been quantified in this way, the stability of accommodation should be studied. The strongest negative glass with which visual acuity is equal 1,0
, leave in front of the eye for
3-5
minutes.
If the stability of accommodation is satisfactory and the accommodative muscle is able to withstand this rather long-term load, then visual acuity will always remain equal to 1.0
(or its original value, if before the study it was less than
1.0
).
If the stability of accommodation is insufficient, the latter quickly relaxes, the caused reflex tension disappears, and the optical system “eye plus glass” again becomes hypermetropic; At the same time, visual acuity decreases. The more hypermetropia increases due to the weakening of accommodation tension, the less visual acuity will be. If we plot time (in minutes) on the abscissa axis, and visual acuity on the ordinate axis, we get a graphical characteristic of the state of accommodation stability. With stable accommodation, the curve will be horizontal; with unstable accommodation, it will be inclined (Fig. 5).
The main advantage of this method is the ability to study the reserves and stability of accommodation while completely excluding the influence of convergence (each eye is examined separately).
↑ Study of convergence, its reserves and sustainability
When studying convergence, it should be taken into account that its maximum tension can be studied by determining binocularly the position of the nearest point of convergence, for which both accommodation and convergence are important. It is interesting that in the process of visual work, the binocular closest point significantly approaches the eyes, remaining in this position even after an hour of rest.
A weak prism is placed in front of one refractively corrected eye (base towards the temple), usually with a force of 10—12
prism diopters (A).
The subject notes the bifurcation of a small lamp located at a distance of 2
to
5
m from him. The prism deflects the beam towards its base. In the eye, the beam falls on the temporal part of the retina, and since in the eye, in front of which there is no prism, the light beam goes to the central fovea of the macula, double vision occurs.
To help the patient notice diplopia, a red glass can be placed in front of the other eye (although this is not necessary). Quite quickly, both images of the lamp merge into one due to additional contraction of the internal rectus muscle of the eye, in front of which the prism is placed.
This contraction is necessary to turn the eye inward so that the light beam deflected by the prism hits the direction of the central fovea of the macula and both beams end up at the corresponding points of the retinas of both eyes. Then take a stronger one (at 2—3?
) prism, diplopia is again obtained, the two images are again achieved to merge into one, and this continues until the strongest prism is found, which can still be overcome with the help of additional convergence caused by the fusion reflex.
With asthenopia caused by weakened convergence, the subject sometimes cannot overcome the diplopia created by applying even a weak prism. by force in 1—:2—3?
. The same thing happens with false and progressive myopia.
To determine the stability of the maximum strength of convergence found in this way, leave a prism in front of the eye for 5
minutes. After every minute, the prism is removed and placed again in front of the eye. With satisfactory stability of convergence, double vision is easily overcome every time; with unstable convergence, persistent diplopia occurs; in the second case, the force of the prism that the subject under study can overcome is determined in the manner described.
If we plot prism diopters on the ordinate axis, and time in minutes on the abscissa axis, we get a graphical characteristic of the stability of convergence. With stable convergence, the curve will be horizontal, and with unstable convergence, it will be inclined (Fig. 6).
In this way, the reserves and stability of convergence are determined independently of accommodation, because the study is carried out at a large distance and for each eye separately.
Structure of the posterior segment of the eye
Vitreous body
Behind the lens is the vitreous body
. The main functions of the vitreous body are maintaining the shape and tone of the eyeball, conducting light, and participating in intraocular metabolism. As a refractive medium it is weak. When examined in transmitted light, the normal vitreous body appears completely transparent.
It has a jelly-like structure in most cases, but sometimes it can become liquefied. On the other hand, compacted areas in the form of threads or lumps may appear in it, the presence of which the patient feels in the form of “flies” and floating dots. In some places, the vitreous body is closely fused with the retina, so when seals form in it, the vitreous body can pull on the retina, sometimes causing its detachment.
↑ Signs of accommodation spasms
An accommodation spasm should be considered an involuntary contraction of the ciliary muscle, i.e. its involuntary tension. Usually spasms of accommodation are bilateral, although cases of “anisospasms” are certainly not uncommon. Spasms of accommodation have been known for a long time. Leading ophthalmologists XIX
centuries recognized their great clinical significance. However, later ophthalmologists stopped paying attention to many signs indicating the presence of spasms of accommodation. As a result, a number of previously known signs of accommodation spasms are now forgotten.
We present in a slightly adapted form the signs of spasms of accommodation described by one of the founders of Russian ophthalmology, E. V. Adamyuk (1881).
- Decreased vision, noticed recently, mostly under the influence of intense exercise.
- Rapid fatigue when working at close range, pain in the eyes and their surroundings, photophobia, increased tear production, desire to bring the book closer to the eyes. These signs of asthenopia appear both with hypermetropia and with increased refraction to myopic with a decrease in visual acuity.
- Reducing the volume of accommodation. E. V. Adamyuk defined it by the distance from the nearest point of clear vision. We have described a more modern and accurate method for determining accommodation reserves (A.I. Dashevsky, 1940, 1962, 1970, 1971).
- In case of myopia, the application of positive lenses causes a deterioration in distance visual acuity; with a spasm of accommodation (false myopia), no deterioration in visual acuity is observed after a short time; sometimes there is a slight increase (due to passive relaxation of the spasm) in visual acuity.
- Attaching positive lenses for true axial myopia forces the text to be brought even closer to the eyes at a close distance. With a spasm of accommodation, reading is possible even at a great distance (due to relaxation of the spasm).
- Repeated determinations of refraction on the same day, and even more so on different days, reveal a constant refraction in case of myopia, and an unstable refraction in case of accommodation spasm.
- E.V. Adamyuk recommends that after determining the refraction, transfer the subject to a dark room for a few minutes and repeat the study again. With myopia, the refraction will remain the same; with a spasm of accommodation, it will be weaker due to relaxation of the ciliary muscle.
- This symptom should be called the symptom of E. V. Adamyuk.
- More than 90
years ago, E. V. Adamyuk paid special attention to the most important symptom of asthenopic phenomena and their consequences - spasm of accommodation - weakness of the internal rectus muscles. True, he did not describe a method for determining the weakness of convergence. The weakness of convergence can best be judged by the state of the convergence reserve (A.I. Dashevsky, 1940, 1962, 1970, 1971). - The main symptom of accommodation spasm is a decrease in refraction at the height of cycloplegia.
Classification of facial muscles
Of course, we won’t tell you about every facial muscle. There are more than a hundred of them! But we will try to explain which muscle groups have the greatest influence on appearance.
Facial muscles
The task of facial muscles is to convey emotion on the face. This occurs due to the extensibility of the skin and the formation of folds that appear across the direction of muscle contraction. This group of muscles is responsible for the appearance of the first wrinkles, which are called facial wrinkles. Moreover, they can occur in youth. Simply because the person is emotional.
Let’s not load your head with terms (each facial muscle has its own name) and divide facial muscles into three types, focusing on their location on the face.
- Muscles of the upper part of the face
Problems: vertical creases between the eyebrows (the pride muscle is responsible for them, which gives a person a frowning appearance), horizontal folds on the bridge of the nose (pyramidal muscle), “crow’s feet” around the eyes (orbicularis oculi muscle). - Muscles of the middle part of the face
Problems: nasolabial lips, wrinkles under the eyes and around the mouth, sunken cheeks. - Muscles of the lower part of the face and neck
Problems: drooping corners of the lips, jowls, swollen oval, marionette wrinkles.
Also, facial muscles can be divided into three groups depending on the direction in which they pull the skin and underlying tissues:
- Depressors.
They pull the fabric down. The pride muscle, which lowers the tissue between the eyebrows and forms wrinkles; muscle that depresses the lower lip; muscle that depresses the nasal septum. - Levators.
Pull the fabric up. The lower part of the frontalis muscle (raises the eyebrows); muscle that lifts the upper eyelid; levator anguli oris muscle; muscle that lifts the upper lip. - Sphincters.
Natural openings are narrowed. Circular muscles of the mouth and eyes.
A simple pattern follows from this classification. Cheerful people have better developed levators, while sad people have better developed depressors.
Chewing muscles
The function of the masticatory muscles is explained by their name. There are four masticatory muscles of the head: the masseter proper, the temporalis, and two pterygoids: the lateral and medial. Also, the neck muscles located above the hyoid bone are involved in chewing movements.
Transformations of the masticatory and pterygoid muscles are especially reflected in the appearance. The masseter is responsible for raising a person's lower jaw when he speaks or eats. The pterygoid muscles help chew rough food. Both the masticatory and pterygoid muscles are tense all the time and are prone to spasms due to excessive clenching of the teeth. The result is impaired blood circulation and, as a consequence, a reduction in the supply of nutrients to cells and skin aging.
↑ Causes of accommodation spasms
Among the causes of spasms of accommodation, E. V. Adamyuk (1881) put in first place blurred vision due to various optical imperfections of the eye (mainly ametropia, clouding of the cornea, vitreous body, etc.), i.e. vision in circles of light scattering.
For better visibility, you have to bring objects closer to your eyes; increased accommodation and convergence can lead to a spasm of accommodation. Poor lighting when working at close range also leads to this.
All causes leading to weakening of the sympathetic or irritation of the oculomotor or trigeminal nerve (due to a reflex effect on the oculomotor) often cause miosis and a parallel increase in accommodation.
Children suffering from chronic intoxication, and therefore a general weakening of the body, usually develop a neurasthenic syndrome, accompanied by irritability, tearfulness, fatigue, sleep disorders, attention exhaustion, etc. With chronic intoxication in children, the balance between irritable and inhibitory processes is disturbed (R.A. Kalyuzhnaya, 1965) with a predominance of either inhibitory states of the cerebral cortex (for example, with a focal infection in the oral cavity and nasopharynx) or an irritable process (for example, with chronic tuberculosis intoxication). This leads to various disorders in the area of the autonomic centers, hypothalamus, endocrine glands, etc.
R. A. Kalyuzhnaya (1965), having studied the functional state of the autonomic nervous system in children during various chronic intoxications, found that with a short time from the onset of tonsillogenic and other intoxications, a high level of sympathetic activity is usually observed; over a longer period of time, sympathetic effects decrease, and a relative predominance of parasympathetic reactions appears. Consequently, with chronic intoxication in children, autonomic dystonia consists of a decrease in sympathetic activity and a relative predominance of parasympathetic activity.
If, due to tonsillogenic, rheumatogenous, tuberculogenic, helminthic, hepatogenic (especially after Botkin's disease) and other chronic intoxications in the body, a predominance of parasympathetic over sympathetic innervation is established, this cannot but affect the state of accommodation of the eye. The predominance of parasympathetic activity (innervation of the Müller muscle) over sympathetic activity (innervation of the Brücke muscle) necessarily leads to the predominance of the accommodation mechanism for near over accommodation at distance.
Under unfavorable hygienic conditions, chronic intoxication, accompanied by vegetative dystonia, expressed in the prevalence of parasympathetic innervation, creates favorable conditions for the occurrence of spasms of accommodation. Therefore, chronic intoxication of the body, especially in children, is one of the most important factors contributing to the development of resistance to spasms of accommodation (V. A. Asabina, 1971).
Among other reasons, special mention should be made of the low reserves of accommodation and convergence identified by E.V. Adamyuk. They are especially low in eyes with astigmatic refraction. Measurement of accommodation and convergence reserves carried out by A.F. Nedelka (1970) in children with astigmatism showed a sharp decrease compared to the age norm.
The occurrence of false myopia is usually attributed to the school period of life. However, cases of pseudomyopia have also been described in preschool children, which is facilitated by the visual load that appears at this age, previous general diseases and many other factors.
The causes of spasms can be divided into the following groups:
- state of the body: intercurrent diseases, chronic intoxication with weakening of the body, vegetative dystonia, ametropia, instability and other disorders of binocular vision, insufficiency of fusional and other functional reserves, etc.;
- environmental factors: poor lighting when working at close range, incorrect posture, bringing the text too close to the eyes, improper daily routine (work and rest), a sharp reduction in time in the fresh air, etc.;
- heredity or hereditary predisposition to spasmodic conditions.
Already V.I. Dobrovolsky (1868) believed that the development of accommodation spasm with emmetropia or hypermetropia contributes to the appearance of visible myopia - pseudomyopia. In his opinion, more 80%
cases of weak myopia (up to
0.5
D) are caused by a spasm of accommodation. At the same time, he reported that with myopia, spasm can be detected at any degree in 60% of cases. He found spasms of accommodation not only with low, but also with high myopia.
The data of V.I. Dobrovolsky were confirmed by Schr?der (1874), who found spasms of accommodation with myopia in 77%
, H?sch and Schiess, who found spasms of accommodation in
81
and
85%
of persons with mild myopia, respectively.
Currently, the opinion about the presence of spasms in a large percentage of cases of myopia is confirmed by many authors. Ticasi Sato (1957) showed in his works the high prevalence of pseudomyopia among Japanese students. K. A. Adigezalova-Polchaeva (1959, 1963) observed spasms of accommodation in 97%
of people with a low degree of myopia, in
72%
a moderate degree of myopia, and in
62%
of people with a high degree of myopia.
Within the framework of the hardware technique, the following is carried out:
- electrical stimulation of the apple of the organ of vision;
- laser treatment at the cellular-molecular level (stimulation of biochemical and biophysical phenomena in the body is carried out - the work of the muscle fibers of the eye returns to normal).
Gymnastic exercises for the visual organs are selected by an ophthalmologist and performed daily for 10-15 minutes. In addition to the therapeutic effect, regular exercise is one of the preventive measures for eye diseases.
Thus, the considered anatomical structure of the organ of vision acts as the basis of the ciliary body, is responsible for the accommodation of the eye and has a fairly simple structure.
Its functional ability is jeopardized by regular visual loads - in this case, the patient is indicated for a comprehensive therapeutic course.
Source
↑ Types of accommodation spasms
Spasms of accommodation are artificial, physiological and pathological (A.I. Dashevsky, 1962, .1968).
↑ Artificial spasm of accommodation
caused by the use of miotics - pilocarpine, eserine, armin, etc.
↑ Physiological spasm of accommodation
caused by contraction of the ciliary muscle to improve distance vision with hypermetropia and astigmatism. This is a long-term tension of the ciliary muscle, which disappears after eliminating the cause of the spasm, i.e., after correcting hypermetropia or astigmatism or eliminating previously allowed overcorrection with negative lenses. The spasm can relax during sleep, with distraction, etc. d.
A distinctive feature of physiological spasm or accommodation tension is an increase in refraction to emmetropia with an increase in visual acuity to 1.0.
↑ Pathological spasms of accommodation
They can be persistent (with ametropia) and true. The former are not true tonic muscle spasms. Tension of the accommodative muscle, caused by the need for self-correction of hypermetropia or astigmatism, is pathological if it becomes persistent. With visual fatigue, persistent spasm can also occur in emmetropes (false myopia), while complaints characteristic of accommodative asthenopia are observed. Persistent spasms of accommodation can only be relaxed with the help of mydriatics or special orthoptic treatment.
The main feature of pathological scasms of accommodation is a decrease in visual acuity due to false myopization.
True spasms of the ciliary muscle are almost always of central origin. With very persistent true tonic muscle spasms of accommodation, it is very rare to achieve full visual acuity with the help of correction.
Continued in the next article.