Myopic astigmatism is a phenomenon that affects about 25% of patients suffering from various pathologies of the organ of vision.
Many patients are interested in how they can be cured of this disease once and for all. Modern medicine involves both traditional and more radical methods of treatment. The choice of a more suitable method is determined individually and depends on the degree of development and clinical course of the process.
Today's article is about myopic astigmatism. The causes, classification, complications, as well as the main methods of treatment and prevention of this pathology of the organ of vision are covered.
Share
Tweet
Share
Cool
Send
What it is?
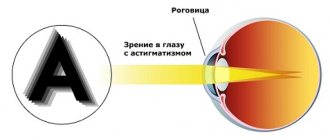
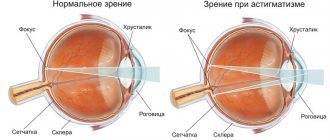
Astigmatism is a pathological vision condition that is associated with a violation of the shape of the lens, cornea and the eye itself. Leads to impairment of the ability to see clearly.
The mechanism of the disease is as follows. The curvature of the cornea or lens of the eye is disrupted, which leads to distortions in vision. Light rays do not converge on the retina at one point. As a result, the image is formed in the form of a blurred segment, a figure of eight or an ellipse.
Causes of astigmatism
According to the nature of its occurrence, astigmatism can be congenital or acquired. In the first case, the disorder can be inherited or occur during the formation of the fetus. If one of the parents had similar vision problems, then the disease at the genetic level can be passed on to the baby. The probability of transmitting a hereditary disease in this case is 50% to 50%. If both parents had ophthalmological disorders, the risk increases to 75%.
During pregnancy, the following factors can trigger the development of eye disease:
- alcohol consumption;
- smoking;
- use of antibiotics.
In addition, the disease can be caused by incorrect position of the muscles, eyelids and bones of the orbit. Due to such pathologies, uneven pressure is placed on the eyes, which leads to impairment.
The most common causes of acquired astigmatism are:
- injuries of the cornea and lens;
- inflammatory diseases (for example, keratitis, blepharitis, etc.);
- consequences of eye surgery, when the patient did not follow postoperative recommendations or the sutures were applied incorrectly;
- degeneration of the cornea, which can result from a disease such as keratoconus: the membrane becomes thinner and takes on a cone-shaped shape.
The main symptom of astigmatism is the distortion of objects. A person sees objects blurred, unclear, or they may appear double.
In addition, visual impairment may be accompanied by:
- headaches;
- painful reaction of the eyes to light;
- poor vision in low light;
- rapid and severe eye fatigue.
A person with astigmatism sees objects blurry at any distance.
Causes
Often, astigmatism develops in early childhood, together with farsightedness or myopia. This condition can finally develop by the first years of life.
As a rule, myopic astigmatism is congenital. This condition is associated either with the inheritance of a pathological defective gene, or with problems that developed during the birth of the child. These include, for example, prematurity.
In addition to congenital causes, it is customary to distinguish acquired ones. These include the following:
- surgical interventions on one or both eyeballs that led to deformation of the eye (for example, after cataract removal);
- traumatic injury to the orbit or the immediate eyeball, which subsequently leads to scars on the surface of the eye;
- dystrophic damage to the cornea (keratoconus), in which the eyeball takes on the shape of a cone;
- impaired blood circulation in the area of the orbit and eyeball;
- exposure to external irritating factors;
- increased intraocular pressure;
- other somatic pathologies (diabetes mellitus, arterial hypertension, diseases of the nervous system).
Myopic astigmatism in both eyes - diagnosis
The degree of astigmatism can be determined only after a thorough diagnosis by an ophthalmologist. The diagnostic process consists of the following procedures:
- Checking visual acuity. To do this, one eye needs to be closed, and lenses (cylindrical) are installed in front of the second, which are characterized by different refractive power indicators. This makes it possible to determine which option is more suitable.
- Skiascopy of the organs of vision. Allows you to evaluate the light reflex of the visual organs.
- Computer refractometry. For the procedure, a special device is used - a refractometer. The duration of the procedure does not exceed 3 minutes. This procedure should be avoided if there is increased intraocular pressure.
REFERENCE! The ophthalmologist may refer the patient for ophthalmoscopy and biomicroscopy.
Classification
As mentioned earlier, astigmatism is divided into three categories:
- complex farsighted;
- complex myopic;
- and mixed.
Varieties
Astigmatism is classified depending on the severity of the pathology, the severity of vision and the involvement of other processes - for example, myopia.
Astigmatism in both eyes
The phenomenon of astigmatism can occur in both eyes or in one. A single process can be caused by inflammatory diseases of the eyeball, traumatic injury or complications after surgery.
Simple
With a simple form of astigmatism, partial visual disturbances are observed - a beam of light reaches the retina of the eye, but the scattering of light rays occurs not at one, but at several points.
Complex type of pathology
In addition to the phenomenon of astigmatism, the complex form is also accompanied by one of the degrees of myopia. The image begins to form at several points before the light beam hits the retina of the eye.
Mixed
The mixed type of astigmatism is divided into three subtypes.
| Mixed myopic astigmatism | Mixed hypermetropic astigmatism | Mixed astigmatism |
| With this type, the two meridians of the eye place rays of light in front of the retina of the eye. | Two meridians place light beams behind the retina. | One meridian focuses light in front of the retina, and the other behind it. |
Degrees
Experts also classify myopic astigmatism into three degrees: weak, moderate and high.
Weak
A weak degree of astigmatism is set to 3 D (diopters). Often not felt by the patient, it is detected by chance during medical examinations or routine vision tests.
Astigmatism
To roughly imagine how a person with astigmatism sees, you need to look at yourself with a teaspoon. This is a disease that is characterized by a defect in the refractive power of the eye, that is, refractive error. The reason is a distortion of the shape of the lens or cornea of the eye.
In healthy organs of vision, the lens and cornea have an even hemispherical shape. With astigmatism, their surface is distorted. As a result, light rays passing through the eyes are scattered incorrectly. Since the rays are not focused at one specific point, part of the image goes to the retina, and part is formed in front of it. A person with astigmatism ends up seeing a distorted picture. Objects at any distance appear slightly blurry. Outlines can stretch both horizontally and vertically. A distorted image is the main symptom of the disease.
Very often, astigmatism is combined with other visual impairments, such as myopia and farsightedness. Depending on this, astigmatism is distinguished:
- Simple. Myopia or farsightedness appears only on one meridian (conventional horizontal and vertical lines perpendicular to each other) of the eyes.
- Difficult. Deviations are characteristic of two meridians.
- Mixed. Myopia appears on one meridian, and farsightedness on the second.
If astigmatism is combined with myopia, it is called myopic. When farsightedness occurs along with astigmatism, it is hypermetropic astigmatism.
Symptoms
The main symptoms of myopic astigmatism include the following:
- decreased vision;
- objects may appear forked or twisted;
- headache;
- a burning sensation in the eyes;
- severe lacrimation and, conversely, increased dryness of the mucous membrane;
- rapid eye fatigue when reading, writing, or working at the computer.
When encountering these symptoms, many patients associate their appearance with prolonged visual work or fatigue. However, if the appearance of such symptoms is permanent, it is necessary to consult an ophthalmologist to rule out this or that pathology. Early detection of the disease allows you to deal with it much more effectively and quickly.
How does a person with pathology see?
A person suffering from myopic astigmatism sees the world somewhat differently from a person with normal vision. The perception of the surrounding world also depends on the degree of astigmatism. With a weak degree, a person may not notice vision problems, or simply get used to such changes.
More pronounced symptoms appear with moderate degrees of astigmatism. The person begins to complain of constant lacrimation and a fuzzy double image. The “picture” that a person sees can worsen at the time of exacerbation of the disease, with fatigue, overwork and mental overstrain.
Objects that are in the background are also distorted in size and shape. A pairing effect can also be observed, in which objects located far away double in size.
Therapy methods
Myopic astigmatism can be completely cured if there is no pathological change in the corneal layers or lens. Two types of therapy are used:
- selection of lenses and glasses;
- surgery.
The initial degree of pathology does not require surgical medical intervention. The patient is prescribed special contact lenses or glasses, and special eye exercises are performed.
Important! Parents need to know that they cannot select glasses for their child on their own. This is done by an ophthalmologist. The glasses will change as the child's visual system changes.
In modern ophthalmology, soft contact lenses are used - toric. They do not cause discomfort when blinking or moving the eyeball. Lenses are prescribed for myopia up to 4D. Lenses are preferable to glasses in every way.
Myopia with astigmatism of a more serious degree of pathology can only be treated surgically. The use of lenses and glasses is harmful - the patient begins to feel dizzy. However, surgical intervention is performed only in adult patients over 18 years of age, when the fundus of the eye is fully formed.
Surgery
Myopic astigmatism in both eyes can be successfully treated with modern surgical methods. After the operation, the patient completely regains his lost vision, the quality is guaranteed for life.
Surgical methods include:
- keratotomy;
- keratectomy;
- laser correction - lasik;
- corneal transplant;
- lens replacement.
Keratotomy is an effective and quick way to restore visual organs. During this operation, the surgeon makes incisions on the cornea, after which the focus of the eyes is completely aligned. Tissue regeneration after surgery occurs in a short time, and the patient gets the opportunity to see an undistorted picture of the world.
Keratectomy is a laser treatment: a directed beam cuts off the top layer of the cornea. This technique has a big disadvantage:
- impossibility of simultaneous correction of both eyes;
- painful rehabilitation period.
Until the cornea is completely healed, you will need to wear special glasses to protect your eyes from light. The effect of the operation is always good, but the eye will take at least six months to heal.
Laser keratomileusis (LASIK) is a partial removal of the upper corneal layer, in contrast to keratectomy. Using a laser beam, pathological areas are burned out and covered with the cornea's own tissue. This method is more gentle than the first. The operation can be done on both eyes at once, and the recovery period is relatively painless within a couple of weeks. No stitches are required with this method.
The actual lens is also implanted under the cornea. The method is suitable for intolerance to conventional lenses. In difficult cases, when laser correction does not help, a donor cornea or an artificial lens is implanted.
Diagnostics
Diagnosis of myopic astigmatism consists of the following studies:
- collection by the doctor of complaints and anamnesis of the disease (how, when and under what circumstances it began);
- objective examination of the eyeballs by an ophthalmologist;
- measurement of intraocular pressure;
- performing biomicroscopy;
- ultrasound examination of the vessels of the brain and orbit;
- visometry is a method that allows you to assess visual acuity;
- determination of the degree of myopia and refraction of a beam of light by the eye.
Myopic astigmatism is diagnosed in two stages:
- vision is checked in the normal state of the eyes;
- vision test with dilated pupils.
Thus, final confirmation of the diagnosis is obtained after testing with atropine. It belongs to the M-anticholinergic blockers, which promote pupil dilation. After this, a skiascopy is performed.
The skiascopy method (shadow test) is necessary to determine the refraction of the eyeball. Based on observation of the movements of shadows in the pupil area. In this case, the eye is illuminated by a beam of light that is reflected from the mirror.
Myopic astigmatism can be diagnosed independently. If you look at a sheet of paper with one eye on which dark parallel lines are drawn, while rotating this sheet, the patient will notice that the lines are either blurred or, on the contrary, become clearer.
Useful video
Myopic astigmatism:
How to distinguish the disease from myopia?
Myopic astigmatism is a combination of myopia and astigmatism. How to distinguish these two conditions? With myopia, the image is focused in front of the retina of the eye, and with myopic astigmatism, the light rays are located at several points.
A distinctive feature of myopia is that it often occurs in childhood and can go away on its own by the age of 20. Myopic astigmatism tends to appear at any age.
High myopia and astigmatism
High myopia and astigmatism Source: pudp.ru A person can receive almost all information about the world thanks to the organs of the visual system.
But people often encounter numerous eye health problems. Today, more and more people have a complex vision defect - high myopia with astigmatism. This ophthalmological disease is called myopic astigmatism. It can affect one eye or both at the same time. The cornea or lens of a patient with high astigmatism has an irregular, distorted shape.
Therefore, there is a curvature of the meridian of movement of light rays penetrating into the eyeball. These rays have abnormal refraction and focusing. Only part of the image of objects is projected onto the retina. Therefore, the reflection of what a person’s gaze is directed at on the retina is distorted.
Ophthalmological diseases are often combined with each other. One striking example is high myopia accompanied by astigmatism. This is a fairly common pathology that is often diagnosed at a very early age.
The disease leads to a severe deterioration in visual functions, resulting in a decrease in a person’s quality of life. The causes and methods of treating pathology are well studied today, so therapy is extremely effective in most cases. It will also be useful for you to find out whether people with complex myopic astigmatism are recruited into the army.
Normally, in a person, the reflection of an object is focused on a specific point of the retina of the eyeball (retina), but with astigmatism it is deformed or the physiology of the cornea or lens is disrupted. Therefore, a ray of light is refracted not at the retina, but in front of or behind it.
Myopia with astigmatism is very common. If the degree of myopia is too high, laser correction cannot be applied. In this case, a combined operation is possible for treatment. First, myopia is corrected by implanting an intraocular lens.
Nearsightedness, also known as myopia, is an eye condition in which a person has trouble seeing objects that are far away. However, he can clearly see objects that are nearby.
Patients with a high degree of this disorder can see clearly only objects located in close proximity to the eyes. In patients with myopia, the eyeball is too long. Because of this, the cornea of the eye is too far away from the back of the eye.
As a result, light rays entering the eye are refracted incorrectly. They focus not on the retina, as they should be, but in front of it. A complex form of this condition is called high (significant or strong) myopia.
Visual impairment is measured in special units - diopters. For myopia, their value is preceded by a minus sign. The higher the number of diopters, the worse the vision. Persons suffering from a high degree of this pathology have more than 6 diopters.
The symptoms of this disease are the same as for lesser myopia. Patients experience eye strain and fatigue when reading or driving, headaches, and squinting of the eyes.
Myopic astigmatism in children
Particular attention should be paid to children, as they generally do not complain of visual impairment. But parents should be wary if the baby squints, looks at images and objects, tilts his head, he often has a headache and his eyes quickly get tired.
If the child is not corrected in a timely manner, the child may develop amblyopia - decreased vision or strabismus. Therefore, early diagnosis is important, which is possible with regular visits to the ophthalmologist.
Important
Serious diseases in the field of ophthalmology include congenital myopia, which appears due to the elongation of the child’s eyeball during its intrauterine development. Hereditary factors play an important role in diagnosis.
The transmission of congenital myopia very often occurs from parents to children if one of them is a carrier of the disease. Children are usually farsighted. The passage of the projection of light rays outside the retina is determined by the short axis of children's eyes.
Over time, this feature of the visual system, which is considered the age norm in young children, goes away. And with congenital myopia in infants, the eyeball has an elongated shape and causes light rays to fall in front of the retina.
Ophthalmological pathology is considered a dangerous disorder in the functioning of the visual organs and negatively affects the general well-being and development of the child.
For parents faced with such a problem, it is important to know about the possibilities of treatment and obtaining positive results after it. An interesting fact is that people with myopia do not experience discomfort when viewing objects at close range.
Disease in children
Myopic astigmatism is quite common among children. It is important for even the most attentive parents to take into account that children can rarely complain about vision problems. If you notice that your child squints when looking into the distance, or can look at an object from different angles, contact a specialist.
Once the diagnosis is confirmed, the child is prescribed treatment. In most cases, this is optical correction using glasses. Contact lenses are not used to correct astigmatism in children.
Gymnastics for children's eyes
Eye exercises are used both to correct the disease and to prevent it. The most effective of them are presented below.
Exercise "Tip"
A red dot is placed on the tip of the child's nose. After inhaling, the child's gaze focuses on the tip of the nose and returns back to its original position. Next, the eyes are closed. The exercise is performed 8-10 times in three approaches.
What is the danger of complex astigmatism and how to treat it correctly
There are several methods of treatment and correction of pathology. The treatment methods are chosen by the doctor, his recommendations must be followed strictly. This is especially true for children, because for them untimely treatment can contribute to the development of dire consequences.
If the degree is weak, conservative treatment is carried out, including optical correction - wearing special glasses or contact lenses and performing exercises for both eyes. In advanced cases, surgical correction is used, since lenses or glasses cause headaches.
Surgical methods give better results. Laser correction is considered the most modern technique. The laser technique takes only 30 seconds to 2 minutes and does not require special rules for recovery after surgery. Treatment methods such as conventional keratotomy and with lens implantation are also used.
Treatment of myopic astigmatism is a difficult and lengthy process. The only method of treating the disease in children is wearing glasses in combination with eye exercises.
What to do if the pathology occurs during pregnancy
Pregnant women should undergo regular examinations at the antenatal clinic at their place of residence. If astigmatism was detected during gestation, it may serve as a contraindication to vaginal delivery. The most acceptable outcome of pregnancy depends on the severity of the disease and the presence of concomitant somatic pathology.
Important! If a pregnant woman has problems with her vision, she must inform her therapist and obstetrician-gynecologist, who are regularly monitored, about this.
Selection of glasses for astigmatism
Description
As already mentioned, rays of light emerging from one point (homocentric rays), lying somewhere throughout the region of clear vision, after refraction in the eye, unite again at one point (remain homocentric).
For spherical refractions
(emmetropia, hypermetropia, myopia) the light beam after refraction in the media of the eye mainly has the shape of a light cone, the apex of which coincides with the main focus of the optical system of the eye; each of these refractions differs from one another in the position of the main focus relative to the retina, but the structure of the light cone does not change and the homocentricity of the rays is not violated.
This position turns out to be true only for spherical refraction, and then relatively.
For astigmatism
rays after refraction in an astigmatic eye are not collected at one focus and therefore the refracted light beam does not have the shape of a cone.
The name itself is astigmatism
(“a” is a negative particle, “stigma” - in Greek - a point (means that rays emanating from one point, when refracted in the optical system of the eye, will not give an image of a point. Instead of a point on the retina, the image of a circle, a straight line ( vertical or horizontal) or oval.
With corneal astigmatism, the cornea has a peculiar curvature. Among its meridians there is always one - with the shortest radius, i.e. with the greatest refractive power, the other - with the longest radius, i.e. with the weakest refractive power.
These two meridians - one with the strongest and the other with the weakest refraction - are called the main meridians. If they are mutually perpendicular and within each of them the refraction is constant, then such astigmatism is called correct, and it is precisely this astigmatism that can be corrected with cylindrical glasses.
Sometimes astigmatism of the eye can be caused by irregular curvature of the lens, which can either increase corneal astigmatism if both are of the same nature, or decrease if both are of the opposite nature. Small degrees of lens astigmatism are quite common, but high degrees are rare.
In Fig. 29 shows the main meridians of an astigmatic eye: the highly refractive vertical meridian AB and the weakly refractive horizontal meridian CD. Refraction of the vertical meridian M 2.0 D, horizontal H 3.0 D. Both meridians are mutually perpendicular. According to the still widespread idea, intermediate meridians have a refraction that gradually transitions from one main meridian to another. This understanding of the conoid, that each intermediate meridian has its own radius of curvature and, therefore, its own refraction, which changes gradually from one main meridian to another, is currently recognized as erroneous.
Astigmatism degree
is expressed by the difference in refraction of two main mutually perpendicular meridians. They can also have an oblique direction, but must always be mutually perpendicular.
The degree of astigmatism expresses only the difference in the refractive power of the two main meridians and does not say anything about the refraction of each of the two main meridians. This difference is determined by simple subtraction. The degree of astigmatism shown in Fig. 29, equal to 5.0 D,
+3.0 D - (- 2.0 D) = 3.0 D + 2.0 D = 5.0 D.
This means that the vertical meridian refracts more strongly than the horizontal meridian by 5.0 D.
With astigmatism, it is necessary to determine two refractions, i.e., the refraction of the strongest meridian and the refraction of the weakest meridian. This is the difficulty of diagnosing and correcting astigmatism.
According to the two main meridians in an astigmatic eye, there are two focal lines and, depending on the location of the latter relative to the retina, the following types of astigmatism are distinguished.
1. Simple astigmatism
, when one of the focal lines coincides with the retina, and the other is either in front of the retina (simple myopic astigmatism - ast. M.) or behind it (simple hypermetropic astigmatism - ast. H.), i.e. one of the main meridians has emmetropic refraction, and the other has myopia or hypermetropia.
For example:
2. Complex astigmatism
when both focal lines are located either in front of the retina (complex myopic astigmatism - ast. MM.), or behind it (complex hypermetropic astigmatism - ast. HH.), i.e., in both main meridians of refraction of the same name, but of different degrees.
For example:
3. Mixed astigmatism,
when one focal line is in front of the retina, the other behind it (ast. MH.), i.e., in one main meridian there is myopia, and in the other there is hypermetropia.
For example:
In the examples given, the vertical meridian has the strongest refraction. This astigmatism is called direct. When the horizontal meridian has the strongest refraction, then astigmatism is called reverse.
The direction of the two main meridians in an astigmatic eye may be different. The direction of the meridians is indicated on the diagrams. The generally accepted system is “Standard”, otherwise called “Tabo” (Fig. 30). According to this system, in the diagrams 0° is placed on a semicircle at the right end of the horizontal meridian for each eye (on the right 0° is at the nasal side, on the left at the temporal side).
The meridians are counted from 0° to 180° counterclockwise, so that 90° is at the upper end of the vertical meridian, and 180° is at the left end of the horizontal meridian. If one of the main meridians has a slope of 45°, then the other meridian should have a direction corresponding to 135° (45° + 90° = 135°). The meridians are counted exactly the same way in both eyes, therefore the designation of meridians in degrees will be the same for each eye.
In most cases, the main meridians have vertical and horizontal directions. In cases of oblique direction of the main meridians, they may have a slope to the temple or to the nose in both eyes, or in one eye the meridian will have a slope to the temple, and in the other to the nose. The different positions of the meridians are illustrated in Fig. 31 and 32.
Astigmatism in most cases is a congenital refractive error that changes somewhat over the course of subsequent life (for example, reverse type astigmatism may increase with old age). Along with congenital astigmatism, acquired astigmatism occurs, which develops due to previous corneal diseases or after operations, most often after cataract surgery.
Strictly speaking, there is not a single eye that would have the same refraction in all meridians of the eye, that is, would not have astigmatism. An ideally spherical surface of the cornea can be found in exceptional cases. Weak degrees of astigmatism (up to 0.5 D) are even called physiological, since they... do not cause any complaints, and therefore in most cases do not require correction.
Only starting from 0.75 D and above, astigmatism reduces visual acuity and causes complaints from patients.
When there is a decrease in visual acuity, and positive or negative lenses do not improve it or improve it only slightly, one has to suspect the presence of astigmatism. Even if there is another reason to explain the decrease in vision, the eye being examined should be checked for the presence of astigmatism, since we are always interested in the visual acuity of the eye with correction of its refraction, including astigmatism.
To diagnose astigmatism, there are subjective and objective methods. Both methods complement each other, and therefore it is necessary to use both.
In the first place among the objective methods should be considered the skiascopy method. The use of skiascopy for astigmatism is described above. After determining the refraction of the main meridians, the degree of astigmatism becomes known and the subjective study and correction of astigmatism can begin.
One of the methods for subjectively determining astigmatism
is the study of the stenopeic fissure. A narrow stenopeic fissure is placed in front of the patient's eye in a trial universal frame, which isolates one of the meridians of the eye. The study begins with the patient himself installing this slit in a position that provides the most distinct visibility of the test fonts. The patient will definitely direct the slit along the meridian in which the refraction approaches emmetropic, and an increase in visual acuity is immediately noted. By attaching spherical lenses, the refraction of the isolated meridian is determined and its direction is noted in degrees, according to the scale of the trial frame. Next, the doctor rotates the slit by 90° (vision immediately deteriorates), and then by attaching positive or negative lenses, the refraction of this meridian is corrected and visual acuity is increased. Thus, the refraction of the two main meridians is established. This method requires the patient to have a lot of attention, patience and the ability to observe and capture the moment when the best visibility of objects is achieved. In practice, this method is rarely used (in this presentation it is mentioned because it can be useful for novice ophthalmologists who have little knowledge of skiascopy).
The most accurate definition of corneal astigmatism
achieved using a Zhaval-Shiets ophthalmometer. You just have to remember that this device only indicates the degree of corneal astigmatism (with an accuracy of 0.25 D) and the direction of its two main meridians, which is counted on a special disk of the device. The data of the Zhaval-Shiets device are usually written as follows: in the first place is the number of the degree of astigmatism in diopters, then a dash is placed and in the second place the direction in degrees of the more strongly refractive meridian. For example, the entry “Zhaval 4.0 D - 70°” is deciphered as follows: the 70° meridian refracts more strongly than the 160° meridian by 4.0 D; the entry “Zhaval 1.5 D - 0°” means: the zero meridian, i.e. horizontal, refracts stronger than the 90° meridian, i.e. vertical, by 1.5 D (reverse astigmatism).
Finally, a fairly accurate definition of astigmatism
is achieved using a refractometer, which indicates the refraction of the two main meridians not only of the cornea, but of the entire eye and gives the direction of the two main meridians in degrees.
After determining astigmatism using one of the above methods, they begin to correct astigmatism using cylindrical lenses. Spherical lenses cannot correct astigmatism, since they only move the focus of the optical system in relation to the retina, and the nature of the structure of the light beam does not change; therefore, they cannot eliminate astigmatism, that is, the difference in refraction between the two main meridians. This requires cylindrical lenses, which, as is known, refract light rays only in a plane perpendicular to the axis of the cylinder; rays of light traveling in a plane parallel to the axis of the cylinder pass without being refracted.
If, for example, a cylindrical lens + 4.0 D is placed with its axis vertical in front of an eye with simple hyperopic astigmatism of 4.0 D with a vertical meridian having emmetropic refraction, and a horizontal one having hyperopia of 4.0 D, i.e.
then this lens will not have any optical effect along the vertical meridian (emmetropia will remain), but along the horizontal meridian it will act as a positive lens, i.e. it will increase the refraction of the horizontal meridian by 4.0 D, which completely corrects the hyperopia present in this meridian by 4, 0 D. As a result, complete correction of this hyperopic astigmatism will be achieved.
Using the property of cylindrical lenses to refract light rays differently in two mutually perpendicular planes, we can always correct astigmatism by increasing the refraction of the weak meridian or decreasing the refraction of the strong meridian. At the same time, we use cylindrical glass to correct all intermediate meridians, since the distribution of radii of curvature and refractive power in different directions of cylindrical glass fully corresponds to their distribution in the optical system of an astigmatic eye. In practice, the essence of astigmatism correction is to determine the two refractions of an astigmatic eye, the difference between them, and to equalize this difference with cylindrical lenses.
When correcting astigmatism, it is imperative to take into account a possible spasm of accommodation; This is a common complication in people suffering from astigmatism, especially at a young age. Accommodation spasm is characterized by the presence of excess accommodation tension and an increase in the refraction of all meridians of the eye. On this basis, extremely diverse changes in refraction arise.
For example, the first study revealed complex myopic astigmatism of 2.0 D:
After atropinization, i.e., with complete rest of accommodation, simple myopic astigmatism of 2.0 D was detected:
An excess of accommodation of 2.0 D changed the nature of astigmatism, turning simple myopic astigmatism into complex myopic.
In another patient, during the first study before atropinization, complex myopic astigmatism of 2.0 D was also determined:
The second study under atropine revealed simple myopic astigmatism of 2.0 D:
The third study under atropine revealed simple hypermetropic astigmatism of 2.0 D:
Finally, with complete rest of accommodation, complex hyperopic astigmatism was established at 2.0 D:
Due to the overstrain of accommodation, complex hyperopic astigmatism turned into complex myopic.
The transformation of simple myopic astigmatism into simple hypermetropic astigmatism after atropinization at a young age is quite common.
It follows that in childhood and adolescence, when selecting glasses for astigmatism, it is necessary to first paralyze accommodation.
Speaking of spherical refraction correction,
We pointed out that in persons whose vision is corrected by spherical glasses, astigmatism of oblique beams occurs when looking in lateral directions. If astigmatism is corrected with cylindrical glasses, astigmatism of oblique beams occurs to an even greater extent, since cylindrical glasses have different refractive powers in different directions; The degree of astigmatism of the oblique beams will also depend on the direction of view.
Astigmatism of oblique beams will be the smallest if the movement of the eyeballs is made in the direction of the axis of the cylinder and reaches its maximum value when movements are made in the direction perpendicular to the axis of the cylindrical glass. Therefore, it is recommended to place cylindrical glasses with the axis horizontal in glasses for near, and with the axis vertical in cylindrical glasses for distance. Whenever possible, this rule should be followed.
Example 1.
There is a simple direct myopic astigmatism of 5.0 D (ast. M), i.e. the vertical meridian has a myopic refraction of 5.0 D, and the horizontal one has an emmetropic one.
This eye has two refractions: in the vertical meridian there is myopia of 5.0 D, in the horizontal meridian there is emmetropia, i.e. the vertical meridian refracts more strongly than the horizontal one by 5.0 D.
The degree of astigmatism is 5.0 D. The refractive equations of both meridians can be achieved with a negative cylindrical lens of 5.0 D, with its axis aligned with the horizontal meridian. Then along the horizontal meridian this lens will not have any optical effect (emmetropia will remain), but in the vertical meridian the optical effect of the cylindrical negative lens will affect the complete correction of his myopia. Both meridians will become emmetropic and correction of astigmatism will be achieved.
The correction is made as follows: cyl. - 5.0 D, ah 0°.
Recently, a new simplified designation for astigmatic lenses has become widespread. The refraction of the meridian with a smaller number of diopters is written first in order, then the refraction of the meridian with a larger number of diopters. After this, a comma is placed and the direction of the meridian to which the first digit refers is indicated in degrees according to the standard system.
How to get rid of glasses, lenses and astigmatism without laser surgery? You will find the answer to this question in Michael Richardson’s “Seeing Without Glasses” technique.
According to the new designation of astigmatic lenses, the prescription should be written as follows:
0 - 5.0 D, 0°.
This entry should be read this way: the horizontal meridian (i.e., zero) does not need any correction; the vertical meridian requires correction with a minus glass of 5.0 D; 0° placed in last place refers to the zero meridian, the refraction of which is indicated in first place.
Example 2.
There is complex myopic astigmatism with myopia in the vertical meridian of 4.0 D, and in the horizontal meridian of 2.0 D.
How to correct this astigmatism?
In this case, there is direct type astigmatism, that is, the vertical meridian refracts stronger than the horizontal meridian by 2.0 D. The degree of astigmatism is 2.0 D (4.0 D - 2.0 D = 2.0 D). To equalize the refraction of both meridians, a negative cylindrical lens, cyl, is placed in front of the eye. — 2.0 D, axis horizontal; then all rays located in the horizontal plane will pass through this lens without refraction (myopia of 2.0 D will remain). In the vertical plane, the lens partially corrects myopia, weakening it by 2.0 D, resulting in the same refraction in both meridians (myopia 2.0 D). A -2.0 D negative spherical lens is then placed in front of the eye to achieve emmetropia in both meridians.
The correction is made as follows:
and according to the new designation of astigmatic lenses:
— 2.0 D — 4.0 D, 0°.
Example 3.
There is complex hypermetropic astigmatism, hypermetropia in the vertical meridian is 1.5 D, in the horizontal meridian is 4.0 D (ast. NN).
In this case, there is direct astigmatism, since the vertical meridian has a stronger refraction than the horizontal one. The degree of astigmatism is 2.5 D (4.0 D - 1.5 D = 2.5 D). For the equation of refraction, a positive cylindrical lens cyl is placed in both meridians. + 2.5 D axis vertical; then there will be no optical effect on the vertical meridian, and the refraction of the horizontal meridian is partially corrected (hyperopia of 1.5 D will be obtained). Thus, correction of astigmatism is achieved, since the same refraction is achieved in both meridians (H 1.5 D). A +1.5 D positive lens is then added to achieve full correction. The correction is made with the following entry:
Example 4.
Mixed astigmatism with myopia in the vertical meridian is 2.0 D, and in the horizontal meridian with hypermetropia is 2.0 D (ast. MH).
In this case, there is direct astigmatism, since in the vertical meridian the refraction is stronger, and in the horizontal meridian it is weaker. The degree of astigmatism is 4.0 D, i.e. +2.0 D - ( - 2.0 D) = + 2.0 D + 2.0 D = 4.0 D. For the refraction equation of both meridians, a cylindrical lens is taken, according to strength equal to the degree of astigmatism. Since positive lenses, as is known, increase refraction, and negative ones decrease it, then to correct this astigmatism, you can take either a positive cylindrical lens + 4.0 D, or a negative one - 4.0 D. The positive lens must be placed with its axis vertical, i.e. in the direction stronger than the refractive meridian, and negative - in the direction weaker than the refractive horizontal meridian. By placing a cylindrical lens cyl. + 4.0 D with the axis vertical, we will increase the refraction of the horizontal meridian by 4.0 D and instead of hyperopia of 2.0 D we will get myopia of 2.0 D, which will achieve correction of astigmatism, since in both meridians there will be myopia of 2.0 D , and adding a spherical lens - 2.0 D, we get emmetropia, i.e. we achieve full correction. By placing a cylindrical lens cyl. - 4.0 D with the horizontal axis, we will weaken the refraction of the vertical meridian by 4.0 D, i.e. instead of myopia of 2.0 D, it will have hyperopia of 2.0 D and in both meridians the refraction will become the same (hypermetropic), and by adding a positive spherical lens + 2.0 D, we achieve emmetropia, i.e. complete correction. This mixed astigmatism can also be corrected with two cylinders (bicylinders). To correct myopia of 2.0 D in the vertical meridian, we take a negative cylindrical lens cyl. - 2.0 D and set the axis horizontally, and then add a second positive cylindrical lens сул. + 2.0 D axis vertically in order to correct hyperopia of 2.0 D in the horizontal meridian. Recipes can be prepared in the following three options:
According to the new designation of cylindrical lenses, the prescription should be drawn up as follows: - 2.0 + 2.0 D, 90°, i.e., reduce the refraction of the strong vertical meridian by 2.0 D, and increase the refraction of the weak horizontal meridian by 2.0 D, to get emmetropia in both meridians; This is what is indicated on the last recipe. So you need to read all the copybooks according to the new designation of cylindrical lenses.
From the above examples, the following general rules for correcting astigmatism emerge.
1. Cylindrical glasses are only sufficient to correct simple astigmatism. For complex or mixed astigmatism, correction cannot be achieved with a single cylinder. To correct complex or mixed astigmatism, sphero-cylindrical glasses are used, combining the properties of both spherical and cylindrical glasses.
2. The selection of glasses for astigmatism is always carried out using a universal frame, which provides the ability to both rotate the glasses and measure the position of the cylinder axis.
3. The correction cylinder is always taken equal to the degree of astigmatism.
4. The axis of the positive cylinder is always placed along the meridian that has the strongest refraction, so that the optical effect of the cylinder affects the meridian with the weakest refraction, increasing this refraction.
5. The axis of the negative cylinder is always placed along the meridian that has the weakest refraction, so that the optical effect of the cylinder affects the meridian with the strongest refraction, reducing this refraction.
We remind you of one more rule that must be applied whenever possible when selecting cylindrical glasses, namely: in glasses for near it is recommended to place the cylinders with the axis horizontal, and for distance with the axis vertical.
Problem 20.
An 8-year-old girl has poor distance and near vision. Right eye: visual acuity 0.05, with correction - 5.0 D; visual acuity 0.35; left eye: visual acuity 0.04, with correction - 6.0 D, visual acuity 0.3.
According to the Javal-Shiets ophthalmometer: on the right eye ast. 2.0 D - 90°, on the left eye ast. 3.0 D - 90°.
Atropinization is prescribed for a week.
When examining with maximally dilated pupils after a week, the following was found.
Skiascopy:
In a study after repeated atropinization for 8 days, the same data were obtained.
Visual acuity of the right eye without correction is 0.03; with glass correction visual acuity 0.6; visual acuity of the left eye without correction 0.03; with correction sph.—5.0 D cyl. — 3.0 D ax 0° visual acuity 0.6.
Diagnosis. Complex myopic astigmatism 2.0 D in the right eye and 3.0 D in the left.
Cyl. — 2.0 D for the right and cyl. — 3.0 D for the left eye is placed with the axis horizontal. In this case, there will be no optical impact on the horizontal meridian. The cylinders will act only on the vertical meridians, partially correcting their myopic refraction; As a result, astigmatism is eliminated and a total refraction for all meridians is obtained - myopia of 5.0 D. Add a spherical lens sph. - 5.0 D and we get complete correction of complex myopic astigmatism in both eyes, i.e. emmetropic refraction.
The found full correction is assigned.
A prescription is written:
Problem 21.
A 9-year-old boy complains of poor vision, especially near.
Right eye: visual acuity 0.05, with correction - 2.0 D, visual acuity 0.3; left eye: visual acuity 0.08, with correction—0.5 D, visual acuity 0.1.
Skiascopy:
Using the Zhaval-Shiets ophthalmometer, it was found: in the right eye, astigmatism 2.0 D - 90°; on the left eye there is astigmatism of 2.5 D - 90°.
Atropinization is prescribed for a week.
During skiascopy with maximally dilated pupils:
Visual acuity of the right eye 0.1; with glasses, visual acuity 0.5; visual acuity of the left eye without correction 0.02; with correction cyl.+ 2.5 D ax 90° visual acuity 0.7.
Atropinization is prescribed for another 3 days, since in the left eye myopia in the vertical meridian has completely disappeared, in the right eye myopia of 1.0 D still remains in the vertical meridian. There is no certainty that the spasm of accommodation has been completely eliminated.
When examined for the third time, 3 days later, with skiascopy, we find the following:
Visual acuity without correction in the right eye is 0.1; with glass correction cyl. + 2.0 D ax 90° visual acuity 0.7; in the left eye, visual acuity without correction is 0.01; .
When examining after additional atropinization, another 3 days later, the same data were obtained.
Diagnosis. In the right eye there is simple hypermetropic astigmatism of 2.0 D; on the left there is complex hypermetropic astigmatism of 2.5 D, with hypermetropia in the vertical meridian of 1.0 D, in the horizontal meridian of 3.5 D. Accommodation spasm.
Making the recipe:
Problem 22.
A 6-year-old girl has poor vision and squints in one eye or the other.
There is a converging concomitant strabismus of 32°.
Visual acuity of the right eye 0.01; with correction + 3.0 D visual acuity 0.4; visual acuity of the left eye is 0.02 with correction + 4.5 D, visual acuity is 0.2.
Skiascopy:
According to the Zhaval-Schiets ophthalmometer: on the right eye ast. 2.0 D - 90°; on the left eye ast. 2.5 D - 90°. Atropinization is prescribed for a week.
When re-examining a week later with maximally dilated pupils, skiascopy:
Visual acuity of the right eye without correction is 0.02; with correction by 90° glasses, visual acuity 0.5 - 0.6; visual acuity of the left eye without correction 0.01; with glass correction, visual acuity 0.4.
When repeating the study after additional atropinization for 3 days, the same data were obtained.
To correct astigmatism in the right eye, we take cy1.+ 1.5 D and, as a general rule, set it as the axis of the strong meridian (90°), which partially corrects the hyperopia of the weak meridian (0°), where instead of hyperopia at 6.5 D we will cause hyperopia 5, 0 D and thus eliminate astigmatism (in both meridians there will be H 5.0 D). By adding a spherical lens + 5.0 D, we achieve complete correction, i.e. emmetropia.
On the left eye cyl. + 2.5 D, placed along the strong meridian (90°), we will reduce the hyperopia of the weak meridian (0°) by 2.5 D and obtain a total hyperopia of 5.0 D in both meridians, thereby eliminating astigmatism. By adding a spherical lens at +5.0 D, we get emmetropia.
Diagnosis. Complex hypermetropic astigmatism and concomitant convergent strabismus.
Due to the presence of strabismus, complete correction is prescribed.
We write out the recipe:
Problem 23.
A 10th grade student complains of poor vision and severe fatigue during classes.
Has poor vision since early childhood. Wears glasses cyl. - 2.0 D ah. 0° from 1st grade of school; Glasses don't help much.
According to the Zhaval-Schiets ophthalmometer: on the right eye ast. 4.0 D - 90°, on the left eye ast. 4.0 D - 90°; Skiascopic: mixed astigmatism in both eyes.
Visual acuity of both eyes without correction is 0.1; with glasses my vision is 0.2; with lens cyl. — 4.0 D with a horizontal axis, we get hyperopia of 1.5 D in both meridians. By adding spherical glass +1.5 D, we get emmetropia in both meridians. Visual acuity of both eyes with this correction is 0.5.
Due to complaints of accommodative asthenopia and the complete discrepancy between the glasses the patient wears and the refraction established by us, atropinization is prescribed for 7 days.
When examined a week later with maximally dilated pupils, skiascopy in both eyes revealed:
After further atropinization for 2 days, the same data were obtained.
Diagnosis. Mixed astigmatism, accommodative asthenopia. Visual acuity of both eyes without correction 0.05; with glasses correction ax 0° visual acuity 0.6.
When examining binocularly, the patient tolerates glasses best with these glasses, the hyperopia will remain undercorrected by 0.5 D. Since this does not contradict the general rules for correcting hypermetropia, we focus on the last correction.
We write out the recipe:
Problem 24.
A 12-year-old boy complains of poor vision and fatigue during activities.
Visual acuity of the right eye without correction is 0.2; visual acuity of the left eye without correction is 0.1. Spherical glasses do not improve vision. According to the Zhaval-Schiets ophthalmometer: on the right eye ast. 4.0 D - 120°; on the left eye ast. 4.5 D - 60°; Skiascopic: mixed astigmatism.
Atropinization is prescribed for a week. We examine with maximally dilated pupils skiascopically:
Atropinization is prescribed for another 3 days. After 3 days, new data were obtained skiascopically.
With further atropinization, after another 3 days, the same data were obtained.
Visual acuity of the right eye without correction is 0.02; left eye 0.01. On the right eye with correction of cyl. + 3.5 D ax 120° visual acuity 0.7; on the left eye with cyl.+4.0 D ax 60° visual acuity 0.7. As a result, instead of mixed astigmatism detected during the first study, after atropinization for 13 days, simple hypermetropic astigmatism was established; myopia in the meridians 120° on the right and 60° on the left eye disappeared. This example once again confirms the need to study children using atropine.
Diagnosis. Simple hyperopic astigmatism with oblique axes.
A prescription is written:
Glasses for permanent wear: right eye cyl. + 3.5 D ax 120° left eye cyl. + 4.0 D х 60° Dp. = 54 mm
The position of the axes in the designation on the prescription form is presented below:
Problem 25.
The patient, 38 years old, complains of poor vision. I never wore glasses.
Visual acuity of the right eye without correction 0.12, with correction + 4.0 D visual acuity 0.3; visual acuity of the left eye without correction is 0.1, with correction + 4.0 D visual acuity is 0.25.
According to the Zhaval-Schiets ophthalmometer: on the right eye ast. 5.0 D - 110°; on the left eye ast. 6.0 D - 70°.
Skiascopy:
For the right eye cyl. + 4.0 D, placed along the axis of the strong meridian (110°), we do not change the refraction of this meridian, but we increase the refraction of the weak meridian (20°) by 4.0 D, i.e. we partially correct hypermetropia, reducing it to 4, 0 D. This eliminates astigmatism and the same refraction is established in both meridians (hyperopia of 4.0 D), which by adding spherical glass + 4.0 D turns into emmetropic. For the left eye cyl. + 5.0 D, with the axis set along the strong meridian (70°), its refraction is left unchanged, and the refraction of the weak meridian (160°) is increased by 5.0 D and we obtain hypermetropia of 4.0 D, i.e., eliminating astigmatism, we achieve hypermetropia of 4.0 D in both meridians. By adding a spherical lens + 4.0 D to the cylinder, we get emmetropia. With these glasses he can read fonts No. 6 and 7 of Sivtsev's tables fluently. The patient is warned that she needs to get used to these glasses, since they are quite strong and that at first it will be difficult for her to wear them. Advice is given on how to get used to glasses, i.e. at first wear them only in the room, then walk up the stairs, then down the street, etc.
We write out the recipe:
Problem 26.
A 33-year-old patient complains of very poor distance and near vision. She has been wearing glasses for a very long time and has never changed them.
When checking the glasses, it turned out that both eyes have spherical glasses -7.0 D. With correction, visual acuity is 0.1.
Visual acuity of both eyes without correction 0.01; with sph correction. — 13.0 D, visual acuity is 0.4.
According to the Zhaval-Shiets ophthalmometer on the right eye, ast. 4.0 D - 100°, on the left eye ast. 3.0 D - 75°.
Skiascopy:
Diagnosis. Complex myopic astigmatism in both eyes with oblique axes.
It is not possible to provide the patient with complete correction of all myopia and astigmatism. She will not be able to wear such glasses due to the sharp transition from glasses - 7.0 D, to glasses - 12.0 and -13.0 D, and even with cylinders. If you add cylinders to the glasses the patient wears, then such a correction will give very little. Therefore, it is necessary to give an average correction. Guided by the subjective testimony of the patient herself, a correction is prescribed.
A prescription is written:
With these glasses, the patient feels well, distance visual acuity is 0.5-0.6; close up reads font No. 6 Golovin - Sivtseva completely freely. By giving this correction, we warn the patient that she must gradually get used to these glasses and not judge them by the first impression, which may be unfavorable.
The position of the axes in the designation on the prescription form is presented below.
—
Article from the book: Guide to selecting glasses | Galkin N.N.
Will they be drafted into the army if they have a disease?
Whether you will be drafted into the army with myopic astigmatism depends on the degree of development of the pathology. Young people with a weak form of astigmatism (from 2 to 4 diopters) fall under category B. With this form, conscripts are required to serve, but not in all, but in certain troops.
In this case, it is necessary to undergo a medical examination every three years. If during this time it is discovered that the young man's vision has improved, he will be called up for military service.
A definite contraindication to military service is considered to be vision of minus (plus) 6 diopters or more.
Treatment
If a patient has a weak degree of myopic astigmatism, the doctor prescribes a set of exercises. Wearing special corrective lenses or glasses is also prescribed. The operation is performed only if the patient himself insists on it. If the visual impairment is significant, then surgical intervention is recommended; 1 of 3 types of operations can be performed:
- Astigmatic keratotomy;
- Laser keratomileusis;
- Photorefractive keratectomy.
For a number of reasons, the above methods may have contraindications or not give a positive result. In this case, intraocular lens implantation, lens replacement, or corneal transplant may be required.
Prevention
Preventive measures to reduce the risk of development and progression of myopic astigmatism include the following:
- regular visits to an ophthalmologist (at least once a year);
- protection of the organ of vision during traumatic types of work;
- compliance with the rules of personal hygiene of the eyes and face in general;
- periodically performing gymnastic exercises for the eyes;
- limiting loads on the organ of vision;
- maintaining a sleep-wake schedule (full sleep);
- proper balanced nutrition, balanced in proteins, fats and carbohydrates;
- timely implementation of doctor's recommendations;
- fortification of food consumed daily;
- compliance with the treatment plan prescribed by the specialist;
- work at the computer in the correct position and with mandatory breaks.
Reasons for development
Most often, the appearance of pathology is hidden in a genetic predisposition. If both parents or one of them suffered from a similar diagnosis, then the child automatically falls into the risk group.
However, the anomaly can be not only congenital, but also acquired. It develops under the influence of a number of factors:
- Damage to the visual apparatus;
- Inflammatory processes affecting the eyes;
- Unsuccessful surgical intervention;
- Adverse environmental influences;
- Poor blood circulation in the organ of vision;
- Increased intraocular pressure;
- Regular eye strain.
Congenital astigmatism develops when the lens is irregularly shaped and forms in the womb. Such a deviation provokes treatment with strong antibiotics during pregnancy without consulting a doctor. An unhealthy lifestyle, bad habits and radiation exposure can also lead to problems with the baby’s eye health.
| Corneal astigmatism is usually diagnosed due to injury to the eye or improper vision correction. The shape of the shell sometimes changes after illness. |
Return to contents
Myopic astigmatism treatment
Today, conservative and surgical methods are used to eliminate myopic astigmatism. The first involves selecting optical correction tools and taking medications. Moreover, glasses or lenses should be selected by the doctor, taking into account all the individual parameters of the visual system.
Surgical intervention helps achieve maximum effect. Laser correction eliminates the disease once and for all, restoring visual acuity in a short time.
Medicines
It is impossible to get rid of myopic astigmatism with medications. They are prescribed to support the visual apparatus and saturate it with useful elements. Complex therapy includes:
- Massaging the collar area;
- Balanced diet;
- Consumption of vitamins and microelements that are beneficial for vision (manganese, zinc).
| Eat more fruits, vegetables, dairy products. Try to get rid of bad habits. |
Optical correction
After making a diagnosis of “myopic astigmatism,” the ophthalmologist first selects contact lenses or glasses to combat the deviation. It can hardly be called a treatment, since optics only masks the disease without eliminating it. However, corrective products help restore clarity of vision and once again enjoy a full life.
Since myopia and astigmatism often coexist, special models should be selected. For the second disease, you will need cylindrical lenses, and spherical ones to mask myopia. Moreover, these parameters should be harmoniously combined in one accessory.
Typically, glasses are the most affordable and sometimes the only option for correcting the disease. They must be used without fail to eliminate the risk of developing amblyopia or strabismus.
Hardware vision correction
The technique solves several problems at once:
- Visual apparatus training;
- Strengthening the muscles of the eye;
- Normalization of blood circulation in the eyes;
- Activation of nutrition of the organ of vision;
- Stimulating normal functioning of the affected eye (or both).
Return to contents
Eye exercises
Of course, gymnastics will not eliminate myopic astigmatism, but it will improve the accommodative abilities of the visual apparatus and relieve tension from it.
- Type with your finger along the lines in the book, follow the movement with your eyes. Then change the magazine to a clean white sheet and repeat the manipulations. Perform the technique ten times;
- Close your weakened eye. Scatter small beads on the surface of the table and try to fold them into any shape. Then repeat the procedure with the second eye;
- On a sheet of white paper, draw a large geometric figure. Repeat the image with your eyes, following the drawing process with your gaze;
- Stick a large circle on the window. Alternately focus your gaze on it, then on the object behind the glass. Repeat fifty times.
| Do gymnastics every day for ten minutes. You can do exercises with your children to prevent eye diseases. |
Surgical treatment
To combat myopic astigmatism, doctors use two methods:
- Keratotomy. Microsurgical intervention, during which several incisions are made on the cornea with a scalpel. After the incisions heal, the shape of the element changes and the process of refraction of light fluxes is corrected. Due to its low effectiveness and long recovery period, surgery is extremely rarely prescribed;
- Laser correction. The optimal way to combat deviations in the functioning of the visual apparatus helps to completely eliminate the disease. During the operation, the laser beam changes the shape of the cornea according to a template previously calculated on a computer. The intervention guarantees a 100% stable result. After the correction, the patient can return to their normal lifestyle after a couple of days. The rehabilitation period ends quickly, the risk of complications is minimal.
Disease prevention
To minimize the possibility of developing congenital myopic astigmatism, follow simple rules:
- Optimize physical activity;
- Balance your diet;
- Every thirty minutes of working at your PC, take a break and do gymnastics;
- Regularly take a course of vitamins with lutein;
- Treat ophthalmic ailments in a timely manner;
- Perform periodic pneumatic massage to relieve eye strain and improve blood circulation;
- Make sure there is sufficient lighting in the work area;
- Alternate loads on the visual apparatus with active recreation.
| Visit your eye doctor regularly for preventive examinations. This will help detect pathology at an early stage. |