Causes
The causative agents of the infection are herpes viruses type 1 and 2, chickenpox virus or herpes zoster virus. All of them belong to the herpesvirus family. You can become infected with the herpes virus type 1 through airborne droplets, through contact with a sick person, or through a kiss. Infection is observed in childhood. The second type enters the body through the genital tract or is transmitted during childbirth from mother to child.
After introduction into the body or after the first episode of herpes infection, the virus remains either on the cornea or in the trigeminal nerve in an inactive state.
Reactivation of the virus occurs if the following risk factors exist:
- Acute respiratory viral infections.
- Hypothermia or overheating.
- Exposure to ultraviolet rays.
- Decreased body resistance.
- Laser effects on the eyes.
- Using certain eye drops to treat glaucoma.
- Taking antibiotics, corticosteroids and antivirals.
- Microtrauma of the cornea, especially when wearing lenses.
- Nervous tension or chronic stress.
- Hormonal imbalance or pregnancy.
- Alcohol abuse.
After the first case of inflammation, herpes keratitis develops again within a year in 25% of cases. If a person has had ophthalmoherpes twice already, the probability of recurrence within a year increases to 50%, if more than two times - to 75%.
Specifics of the disease
Herpes simplex virus type 1 affects the skin, especially along the nerves, and mucous membranes. The severity of ophthalmoherpes depends on the properties of the virus and the immune response. Herpes affects the eye membranes after it overcomes their protective barrier, consisting of substances in the tear fluid: the natural antiviral substance interferon and protective immune particles - secretory mucus immunoglobulins (IgA).
The herpes virus enters the eye tissue from the external environment, along nerve fibers or through the bloodstream. It actively multiplies on the cornea, causes cell damage and triggers an inflammatory reaction. Corneal cells undergo degeneration, are destroyed and desquamated. If only the surface layer of cells is affected, the tissue defect is restored, and the virus goes into dormant mode.
If the corneal connective tissue is involved in the process, as is observed with deep keratitis, direct damage to cells by the virus itself and additional damage by immune cells occurs. The virus is able to imitate the structure of corneal cells, so the immune system attacks not only viral particles, but also corneal cells.
Inflammation caused by herpes simplex virus type 2 develops in 1 in 500 babies under 6 months of age because the mother passes on antibodies to the virus to her baby during pregnancy.
Symptoms of the disease
Keratitis is characterized by the so-called corneal syndrome, that is, signs of irritation of the cornea. The symptoms of herpetic keratitis at the onset of the disease are difficult to distinguish from signs of bacterial inflammation. The patient experiences:
- Tearing.
- Photophobia.
- Spasm of the century.
- Redness of the eye membranes.
- Sensation of a foreign body in the eye.
- Discomfort, stinging or pain.
At this stage, healing can occur without changing the tissue structure. If the disease progresses or recurs frequently, the virus penetrates into the deeper layers. The skin around the eyes and eyelids become covered with blistering rashes. As a rule, one eye is affected. The blisters quickly burst, and in their place ulcerations form.
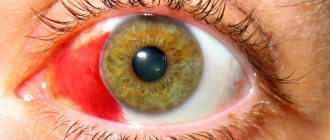
Often herpes keratitis is combined with acute conjunctivitis - inflammation of the outer membrane of the eye. With this course, the parotid lymph nodes may become enlarged.
Symptoms
Different forms of keratitis may present in different ways. With epithelial, or superficial, keratitis, pain, redness and burning appear in the eyes. Patients say they feel as if something is in their eye.
With stromal keratitis, the sensitivity of the cornea decreases and intraocular pressure increases. There is also a sensation of the presence of a foreign body, watery blisters appear and the choroid of the eye is affected.
The primary process is manifested by general malaise, increased body temperature and damage to the upper respiratory tract. Blepharoconjunctivitis may also develop, which progresses favorably and resolves spontaneously. With post-primary inflammation of the cornea, discomfort appears in the eyes, tear production increases, and vision deteriorates.
Herpes keratitis ranks first in frequency and severity among other types of corneal inflammation
Forms of herpetic keratitis
Inflammation of the cornea caused by the herpes virus can be primary and repeated or post-primary. Primary ophthalmoherpes occurs when the body does not yet have antiviral antibodies. As a rule, the infection first develops in children under 5 years of age; less commonly, the primary form occurs between the ages of 16 and 25 years.
The peculiarity of primary ophthalmoherpes is its severe course, a tendency to general intoxication of the body and concomitant damage to the skin or oral cavity. Post-primary herpetic keratitis is sluggish.
There are superficial and deep forms of repeated inflammation of the cornea caused by herpes. Superficial includes vesicular and dendritic keratitis. Deep or stromal - metaherpetic and discoid.
Vesicular form
With vesicular keratitis, grayish blisters form. Due to the appearance of ulcers, the epithelium exfoliates at the site of the opened blisters. In this case, tissue nutrition sharply deteriorates, the regeneration process proceeds slowly, as a result of which the sensitivity of the cornea decreases and it becomes cloudy. The lesion is usually unilateral, but the infection often recurs.
Arborescent keratitis
With this form, severe pain develops in the initial stage. The patient is bothered by severe photophobia, and sometimes “spots” appear before the eyes. Gradually, bubbles form on the cornea. In place of the merged bubbles, gray furrows form. Because of them, lightning and spots appear in the field of vision.
Inflammation provokes detachment of the surface layer, forming ulceration. Tree inflammation occurs over a long period of time and in a sluggish form, complicated by inflammation of other eye membranes, impairing vision and causing significant clouding of the cornea.
Metaherpetic keratitis
It usually develops after a tree lesion, especially if the disease is not treated on time or the wrong doses of hormonal drugs are prescribed. With this deep variant of ophthalmoherpes, the area ulcerated during tree-like inflammation is rejected, and the area of inflammation gradually increases and deepens.
The cornea swells, hardens, becomes dull gray, and then becomes covered with numerous erosions or ulcers. Gradually, white scars form at the site of erosion.
Disc type
This option proceeds slowly, the symptoms are moderate. But fluid accumulates in the cornea and becomes infected. Because of this, the central part of the membrane is damaged, which causes pain in the eyeball.
Gradually, the swelling thickens, and in its place, gray-white foci with clear contours form, consisting of scar tissue; there are no ulcers. The denser the cornea becomes, the less sensitive it is and the more intense the pain. Compacted tissue refracts light worse, which leads to vision impairment.
Keratoiridocyclitis
This variant is characterized by simultaneous inflammation of the cornea and iris, which determines eye color. The patient experiences tingling sensations and sudden attacks of eye pain. The pain is associated with irritation of the trigeminal nerve, so it can spread to the forehead or temples.
A small network of blood vessels is affected, and as it progresses, purulent fluid may leak from the eye. If the process continues, intraocular pressure increases. The pupil is dilated, and when examined, a halo is visible around it.
Treatment of viral keratitis
Treatment of viral keratitis is carried out in a hospital. Its duration ranges from 2 to 4 weeks. Methods of local and general (systemic) therapy are used. The earlier treatment of herpetic keratitis begins, the greater the chance of successful completion. A delay of 1–2 days can lead to significant loss of vision or even death of the eye. It is taken into account that epithelial (superficial) keratitis is caused by live viruses, and deep (stromal) keratitis is an immune reaction to an infectious factor and the result of the inability of the corneal epithelium to heal (development of a metaherpetic ulcer).
The main directions in the treatment of herpes infection are:
- Antiviral and pathogenetic therapy.
- Correction of all parts of the immune system.
Antiviral therapy
Antiviral drugs include Acyclovir, Valacyclovir, and Ganciclovir. The leading place is occupied by Acyclovir. For severe recurrent ophthalmoherpes, Acyclovir or Valacyclovir are prescribed orally. In other cases - local ointment Acyclovir (Zovirax, Virolex, Gerpevir, Ciclovir), Oxolinic, Florenal, Tebrofenov, Bonafton, Kerecid in the form of drops.
Deoxyribonuclease inhibits the synthesis of viral DNA and delays the reproduction of DNA-containing viruses. The herbal drug Proteflazide has antiviral activity.
Pathogenetic therapy
Among the means of nonspecific immunotherapy for the disease, interferons and its derivatives (Lokferon, Reaferon, Oftalmoferon, Okoferon, Laifferon) are widely used. Good results are obtained from the use of interferon inducers (Poludan, Cycloferon).
Immunomodulators (Levamisole, Thymus preparations) are used both parenterally and orally.
Absorbable and anti-inflammatory therapy:
- Dexamethasone is used as a corticosteroid.
- From the group of non-steroidal anti-inflammatory drugs, Diclofenac (Diclofen-F, Uniclofen, Uniclof, Diclof, Naklof), Indomethacin (Indocolir) are used.
Antiallergic therapy: Diphenhydramine + Naphazoline, Ketotifen, Olopatadine.
Stimulators of corneal regeneration: Kornegel, Solcoseryl, solutions Taufon, Taurine, Thiatriazoline, Quinine hydrochloride.
In order to prevent the development of a secondary infection, broad-spectrum antibiotics are used locally: solutions of Levomycetin and Gentamicin, Tobramycin, Tsipromed, Ciprofloxacin, Cycloxan, Lomefloxacin, Floxal, Oftaquix, Vigamox, etc. Tetracycline and Erythromycin ointments are placed behind the lower eyelid.
To prevent the development of iridocyclitis, mydriatics are used.
Antihypertensive therapy: Dorzolamide, Brinzolamide, Timolon, Acetazolamide orally.
In the treatment of ophthalmoherpes, laser coagulation and cryotherapy are used.
Physiotherapy includes electrophoresis with lidase, potassium iodide, etc., diathermy, microwave therapy, and phonophoresis.
If there is no effect, surgical treatment methods (keratoplasty) are used.
Treatment of superficial herpetic keratitis
- Antiviral therapy: Acyclovir, Ganciclovir, Human Interferon.
- Reparative agents: Taurine, sulfated glycosaminoglycans, Dexpanthenol, etc.
- Antioxidants: Methylethylpyridinol.
- Antiallergic therapy: Diphenhydramine + Naphazoline, Ketotifen, Olopatadine.
Treatment of deep (stromal) herpes keratitis without ulceration
- Antiviral therapy: Acyclovir, Ganciclovir, Human Interferon and its derivatives.
- Anti-inflammatory therapy: Dexamethasone in the absence of ulcerations.
- Antihypertensive therapy: Dorzolamide, Brinzolamide, Timolon, Acetazolamide orally.
- Antiallergic therapy: Diphenhydramine + Naphazoline, Ketotifen, Olopatadine.
- Resorption therapy.
Treatment of deep (stromal) herpes keratitis with ulcerations
- Antiviral therapy: Acyclovir, Ganciclovir, Valacyclovir, Human Interferon.
- Corticosteroids are contraindicated in the acute phase of inflammation, in the subacute phase - Dexamethasone parabulbarly 1 - 3 times a week, with complete epithelialization - Dexamethasone daily, gradually increasing the number of instillations to 3 times a day.
- Antibiotics locally or systemically.
- Anti-inflammatory therapy.
- Decongestant therapy.
- Antihypertensive drugs.
- Desensitizing therapy.
- Mydriatics.
Rice. 21. In the photo, the superficial form of herpes keratitis is dendritic keratitis.
Diagnostics
Diagnosis of herpetic keratitis begins with examination. The presence of characteristic blisters suggests a lesion caused by herpes. Since the disease can be sluggish, without characteristic manifestations, the diagnosis is clarified using laboratory and instrumental studies. To detect the pathogen, scrapings are taken from the affected tissues or tear fluid.
Laboratory diagnosis of ophthalmoherpes includes:
- Study of scrapings from the conjunctiva using fluorescent antibodies.
- Linked immunosorbent assay.
- Blood or tear fluid test for antiherpetic antibodies.
- Polymerase chain reaction (PCR) of biological fluids that detects the virus.
Instrumental examination helps to assess the extent and depth of anatomical changes. Instrumental diagnostics include anterior optical coherence tomography, biomicroscopy and fluorescein test.
A fluorescein test is performed to identify ulcers or films on the cornea and assess the area and extent of the lesion. After applying the solution to the eye, the ophthalmologist examines the tissue using a slit lamp with a blue filter.
Diagnostic features
Herpetic keratitis is a disease that requires careful diagnosis. The doctor may suspect a disease based on the clinical picture, but before starting treatment it is necessary to obtain laboratory confirmation of the diagnosis. For this:
- if primary infection is suspected, an intradermal test with the HSV vaccine is performed;
- perform scraping and evaluation of epithelial cells from the cornea;
- do an analysis of tear fluid;
- measure intraocular pressure in the ophthalmologist’s office using a special device;
- in the primary form, serological tests are performed to show the titer of antibodies to viral particles;
- PCR is performed - a study with the help of which it becomes possible to determine the DNA of the herpes virus in the biomaterial, to understand which strain of the pathogen provoked the disease.
An important diagnostic step is to determine how affected the cornea is. To do this, a special substance is instilled into the patient’s eyes, capable of causing harmless temporary coloration of the element. Depending on the degree of staining of different areas, conclusions are drawn about how active the disease is.
Treatment methods
The method of therapy depends on the severity of the disease, the form and time of contacting a doctor. In the initial stages, symptoms can be effectively eliminated and recurrences can be prevented using conservative or non-surgical treatment.
In severe cases, surgical correction of the consequences of ophthalmoherpes is performed. The main goal of therapy is to stop the spread of the corneal defect and stimulate the healing of ulcers.
Conservative treatment
Conservative therapy includes medications and physical therapy. Suitable for eliminating superficial forms of the disease. Mild forms can be treated at home; moderate and severe forms are treated in the ophthalmology department.
Herpetic keratitis of the eyes is treated with the following medications:
- Antiviral drugs.
- Wound healing agents.
- Antioxidants.
- Antibiotics.
Antibiotics are used if there is a risk of bacterial infection, as indicated by purulent discharge from the eyes. Since herpes causes an autoimmune reaction, antiallergic and anti-inflammatory therapy is carried out, especially with frequent exacerbations. The basis of immunological correction is corticosteroids or analogues of adrenal hormones.
For acute infection, instillations, ointments and cleansing solutions for rinsing are used locally. At the same time, it is important to moisturize the mucous membrane in order to prevent dry eye syndrome that occurs when using hormonal, anti-inflammatory or antibacterial agents.
Anti-dry eye products include Gilan Ultra Comfort moisturizing solution. It is identical to natural tear fluid and has no toxic effect on tissue. It can be instilled up to 6 times a day.
To restore the transparency of the cornea, drugs are administered through physical therapy. For herpetic keratitis, electrophoresis with medicinal solutions is used.
Surgery
Surgery is performed if medications and physical therapy do not help, and the corneal ulcer does not heal, affects the deeper layers, or is at risk of rupture. In case of unexpressed changes, the doctor removes the damaged layers by scraping. But in case of severe structural changes, keratoplasty is performed.
Under local or general anesthesia, the damaged cornea is completely or partially replaced with a donor one. After sewing on a new cornea, proper care is required. Rehabilitation lasts about a month, but the process of tissue restoration can be accelerated using local remedies. To prevent infection from entering the operated eye, it is necessary to maintain its moisture.
As a rule, after infections or operations, the secretion of tear fluid is temporarily impaired. Dry eyes can be eliminated with the help of “artificial tears,” for example, Gilan eye drops, which contain sodium hyaluronate. It is able to bind water molecules, preventing the eye membranes from drying out.
Treatment
It is difficult to describe the method of treating a patient and how long it will last, because everyone has their own form of the disease and the causative agent. If the penetration into the cornea is shallow, the doctor will prescribe drugs with selective antiherpetic properties. For example, he will insist on installing a 0.1 percent solution of herplex or stoxyl .
Frequency of use – 8 times/day. The duration of treatment is ten to fourteen days. If treatment is not stopped after 14 days, the corneal epithelium will suffer due to the acute effects of toxins. Therefore, along with stoxyl solution, it will be recommended to use 3% Virolex ointment, but not more often than 4 times a day.
The ophthalmologist will advise the patient to stop taking licopid and its analogues . It is better to replace these immunomodulators with vitamins. It is advisable to take vitamin A, C and inject vitamins B1 and B2 into the muscle.
Reference! If the disease is advanced, ointments are prescribed the same as for the treatment of superficial forms. Immunomodulators are already helping, and injections of B vitamins into the muscle are becoming regular.
Discoid keratitis is treated with leukocyte alpha-interferon or analogues. They may assign a half-dan. Any of the medications is taken by injection . The doctor selects the dosage, taking into account the patient’s health and the severity of the disease.
Epithelial keratitis
Epithelial keratitis is a disease caused by a viral infection that affects both eyes . A person is sick for weeks, months, years, and only when the deep layers of the cornea are affected does he consult a doctor. Upon examination, the ophthalmologist notices slightly raised gray dotted spots.
They do not change color when stained with fluorescein. To confirm the diagnosis, he instills a solution of rose bengal, and they change their color to red. Superficial keratitis is treated immediately when symptoms appear with steroids in installations.
Stromal
Stromal keratitis is a disease that destroys the cornea due to the fact that the herpes virus penetrates deep into it. Because of it, scars appear on the cornea, vision becomes worse and soon a person may simply lose it. This form of the disease develops due to a delayed reaction of the human immune system to the virus. In the USA, it is precisely because of this that scars often form on the cornea.
Attention! It is difficult to protect yourself from this disease. Why? Because it is transmitted from person to person. Once ingested, it never leaves the body and makes itself felt in case of problems with the immune system. Even after a cold or injury, it can appear.
Metaherpetic ulcer
Metaherpetic ulcer is a disease that is considered a kind of transitional form . It develops against the background of the fact that the body is weakened, as a result of which its resistance is reduced. The ulcer affects the cornea more deeply. The cornea is infiltrated around it. Because of this, the epithelium swells, which is also raised. Iridocyclitis completes the clinical picture.
The patient does not suffer from pain and is sometimes unaware of his eye problems. To cure the patient, they prescribe artificial tears, eye drops, and drugs that stop the toxic effect. The ophthalmologist performs punctal occlusion, makes a contact lens band, and transplants the amniotic membrane. As a result, he manages to restore the corneal epithelium.
Complications
With herpetic keratitis, the infection is complicated by the ingrowth of blood vessels into the cornea or its clouding. In severe cases, the affected tissue peels off. A deep ulcer can tear tissue, and clouding can sharply reduce visual acuity.
In severe cases, the eye tissues can become severely deformed within 1-2 days, and the person can lose vision. But in most cases, the process occurs subacutely, gradually destroying tissue. Inflammation can lead to damage to the anterior choroid and swelling of the macula, the central part of the retina.
After surgical treatment, the new cornea may not take root. There is a risk of developing cataracts after surgery. But in almost 90% of cases, keratoplasty does not cause complications.
Diagnosis of the disease
For herpetic keratitis, an ophthalmologist examines the eye to determine the location, size, and depth of the inflammatory process. Afterwards, laboratory tests of the biomaterial from the eye are prescribed. Comprehensive diagnostics involves:
- Biomicroscopy. The anterior segment of the eye is examined using a slit lamp.
- PCR diagnostics. During the procedure, the genetic material of the pathogen is analyzed.
- Scraping from tissues of the conjunctiva and cornea.
In the following video, an ophthalmologist will talk about how to diagnose an eye infection:
Preventive measures
Prevention of herpetic eye damage includes strengthening the immune system and administering vaccines. To avoid repeated episodes of inflammation, it is recommended to avoid hypothermia, emotional or physical stress, and take immunostimulants and vitamins during the season of acute viral infections.
When wearing contact lenses, it is important to properly care for them: remove them at night, clean them with solutions, and do not place them on your eyes after the expiration date.
The most effective method of prevention, however, remains vaccination.