If the retina is torn or detached, surgical treatment is prescribed to restore the integrity of the eye tissue. The operations are performed under the control of a microscope; they are considered highly accurate and quite complex. Despite this, almost all patients achieve positive results when performed early. The duration of restoration of intraocular structures depends on the type of damage, the age of the patient, and the method of intervention.
Classification of retinal dystrophy
Retinal dystrophy is divided into two large types. These are hereditary and acquired forms of the disease. If we talk about hereditary dystrophies, then destruction occurs at the level of receptors that allow vision in the twilight. The following types of hereditary lesions are distinguished:
- Generalized - degeneration of the pigment type, congenital blindness or lack of night vision, impaired or absent color perception.
- Peripheral - retinal separation due to the characteristics of chromosomes, damage to connective tissue, dysfunction of the rod and cone systems.
- Central - hereditary macular degeneration with the appearance of spots or yellow lesions, dystrophy against the background of age-related changes.
If we talk about the secondary (acquired) form of retinal dystrophy, it is also divided into peripheral and central. The disease of the central type is in turn divided into wet and dry manifestations of dystrophy. In the first case, the formation of new vessels is observed in the affected area. They are very fragile, so elements contained in the blood leak through them. As a result, edema forms and the light-sensitive elements of the visual organs are damaged. This disease is severe, so increased attention is paid to its treatment.
Dry central retinal dystrophy occurs in 90% of cases. It becomes the result of a metabolic disorder. In this case, accumulations of products involved in metabolism form between the retina and the vessels.
Peripheral dystrophy
This manifestation is typical for myopic people and very often leads to retinal detachment. There are two types of peripheral dystrophy: chorioretinal and vitreoretinal. Peripheral chorioretinal dystrophy (PCRD) affects the membranes of blood vessels. Peripheral vitreochorioretinal dystrophy (PVCRD) affects the condition of the cornea. In addition, peripheral dystrophy can be cystic, frost-like and lattice.
Retinal detachment - what is it?
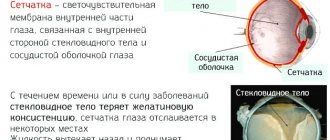
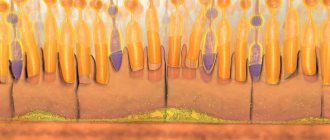
Retinal detachment is a dangerous condition in which, under the influence of many factors, its pigment layer is separated from the neuroepithelium (rods and cones). This process can be painless. Therefore, sometimes the patient does not suspect eye pathology for a long time. This is what leads to irreversible loss of vision.
Causes of retinal dystrophy
The causes of dystrophic changes in the retina can be the following factors:
- Scar formation as a result of disruption of the vascular system or decreased local immunity.
- Non-compliance with diet and consumption of unhealthy or low-quality food.
- Bad habits, in particular smoking and excessive consumption of alcoholic beverages.
- Negligence in the treatment of infectious diseases.
- Presence of chronic diseases. This could be diabetes, blood pressure surges, diseases of the cardiovascular and endocrine systems.
- Eye surgeries.
- Obesity as a result of metabolic disorders.
These manifestations worsen the condition of the circulatory system and slow down metabolic processes. Because of this, the retina is affected. Here's what they say about the causes of retinal dystrophy on the Internet:
Forecast
Detection of pathology requires immediate surgical treatment. Delay in treating this pathology is fraught with the development of persistent hypotension and subatrophy of the eyeball, chronic iridocyclitis, secondary cataracts, and incurable blindness.
The main goal of treating retinal detachment is to bring the layer of photosensitive receptors closer to the pigment epithelium and create an adhesion of the retina with the underlying tissues in the area of the rupture.
In surgery for retinal detachment, extrascleral and endovitreal techniques are used: in the first case, the intervention is performed on the scleral surface, in the second - inside the eyeball. Extrascleral methods include filling and ballooning of the sclera.
Extrascleral filling involves suturing a special silicone sponge (seal) to the sclera, which creates an area of scleral depression, blocks retinal breaks and creates conditions for the gradual absorption of fluid accumulated under the retina by capillaries and pigment epithelium.
Options for extrascleral filling for retinal detachment can be radial, sectoral, circular (circlage) filling of the sclera.
Ballooning of the sclera in case of retinal detachment is achieved by temporarily suturing a special balloon catheter into the area of projection of the rupture; when inflated, an effect similar to filling occurs (a shaft of scleral depression and resorption of subretinal fluid).
Endovitreal treatments for retinal detachment may include vitreoretinal surgery or vitrectomy. During the process of vitrectomy, the altered vitreous body is removed and special preparations (liquid silicone, saline solution, special gas) are introduced instead, which bring the retina and the choroid closer together.
Gentle methods of treating retinal detachment include cryocoagulation of breaks and subclinical retinal detachments and laser coagulation of the retina. allowing to achieve the formation of chorioretinal adhesions.
Cryopexy and laser coagulation of the retina can be used both for the prevention of retinal detachment and for therapeutic purposes alone or in combination with surgical techniques.
The prognosis depends on the duration of the pathology and the timeliness of treatment. Surgery performed early after the development of retinal detachment usually promotes a favorable outcome.
In most cases, retinal detachment can be prevented. For this purpose, patients with myopia, retinal dystrophy, diabetes mellitus, head and eye injuries need regular preventive examinations by an ophthalmologist.
An examination by an ophthalmologist is included in the standard of pregnancy management and helps prevent retinal detachment during childbirth. Patients at risk for retinal detachment are contraindicated in heavy physical activity, heavy lifting, and playing certain sports.
When areas of retinal dystrophy are identified, cryopexy or laser coagulation of the retina is performed for preventive purposes.
Types of retinal detachment
There are central and peripheral retinal detachments.
- With peripheral or marginal vision, deterioration and loss of vision begins around the circumference, that is, from the edges. In the morning the symptom is usually mild and intensifies in the evening.
- Central is characterized by the loss of words, letters, and entire parts from the text being read.
It can also be mobile and rigid.
- Mobile – a milder condition in which, with bed rest for several days, the detached part fits into place.
- Rigid is an unfavorable form of the disease in which such adhesion is absent.
Recovery period
Laser coagulation has virtually no restrictions in the postoperative period. The only thing the doctor can advise is to regularly perform special exercises to strengthen the eye muscles. You should also avoid strenuous physical activity for several months after surgery.
When filling, the list of recommendations is more extensive:
- In the first few days after the intervention, it is necessary to wear a special bandage consisting of two-layer gauze;
- For a month, it is prohibited to lift weights weighing more than five kilograms;
- Do not put pressure on the organ of vision or rub it;
- Avoid getting soapy water into the operated eye;
- Try not to strain your eyes for long periods of time. Limit the period of work at the computer;
- On a sunny day, be sure to wear UV protective glasses.
After vitrectomy, there are a number of other restrictions:
- It is forbidden to expose the visual apparatus to sudden changes in temperature;
- You cannot visit the sauna; use warm water to wash your hair;
- If gas is injected instead of the vitreous, it is not recommended to go down to the subway.
Restoring vision after surgery for retinal detachment depends on the individual characteristics of the body and how quickly the regeneration processes occur in it.
| On average, the effects of surgery disappear within ten days, but in some cases recovery takes months. |
Return to contents
Symptoms of retinal dystrophy
Common signs for all types of retinal dystrophy are the following manifestations:
- Absence or decreased color perception.
- The appearance of image defects (floaters, lightning, flashes, fog).
- Loss of central vision.
- Perception of objects located to the side as a fuzzy picture.
- Decreased visual acuity.
- Loss of sense of movement. An object at rest is difficult to distinguish from one that is moving.
- Need for excessive light while writing or reading.
If we talk about individual forms of the disease, peripheral dystrophy is expressed by the appearance of flashes and dots before the eyes. Damage to the macula is accompanied by curvature of the visible lines. Dry retinal dystrophy distorts visual images. The patient cannot work with small objects and fonts. He has difficulty seeing in the dark and distinguishing faces.
Here is one example of the development of retinal dystrophy and its treatment:
In most cases, the manifestation of symptoms is characteristic of one eye. In addition, the initial stages of retinal dystrophy occur unnoticed. Having discovered the first signs indicating the onset of the disease, you should immediately consult a doctor.
Retinal dystrophy during pregnancy
During pregnancy, retinal dystrophy occurs due to decreased blood flow to the eyes as a result of low blood pressure. If the development of the disease is not stopped in time, it can lead to retinal rupture or detachment. To avoid such consequences, a planned caesarean section or laser coagulation procedure is performed. Laser coagulation is prescribed before the 35th week of pregnancy. The procedure involves creating a reliable connection between the choroid and the retina. The result of such an intervention is to reduce the risk of complications on the visual organs during natural childbirth.
Make an appointment and ask a question:
How can you help in case of diagnosable detachment?
The only way to help is surgery, and urgently.
. If you do nothing, then complete loss of vision is almost guaranteed!
In the center of the eye is the macular zone of the retina, where the largest number of “pixels” are collected; in this zone we see most brightly and clearly. Retinal detachment usually begins from the periphery, and if it has not yet “reached” the center, then with successful surgical treatment the same vision may be preserved as before the detachment. For example, as it was 100% after correction, it remains the same after surgery. If the detachment has already passed through the central zone, then even with successful surgery, central vision is not restored to 100% as usual, in addition, curvature of lines and objects in the center may remain. That is, you cannot delay; under certain conditions, a detachment can reach from the periphery to the center in literally hours!
As with any damage, our body, when the retina is detached, starts the process of inflammation, the formation of connective and scar tissue. And this is very bad for the retina; screeds and scars begin to form on it and under it. It is still possible to help in this case, but the operations become more complex and sometimes multiple. In such cases, vision is also restored, but not to the level it was before retinal detachment.
If thinning of the retinal tissue is diagnosed in time, what treatment is used?
Laser exposure is used. Today this is the only effective method. The essence of the procedure is to create a microburn at the site of thinning tissue, which is then healed and thus these scars create a kind of “dam” around the site of thinning or pre-rupture. This significantly reduces the likelihood of complete retinal rupture and detachment. Moreover, scars form within two to three weeks, and reliable fixation occurs.
It is important to undergo a timely examination of the fundus to identify thinning and prevent rupture in time. For this purpose, special devices are used; such diagnostics cannot be carried out with the naked eye; directional light and special lenses are required.
After 40 years, you need to be diagnosed by an ophthalmologist regularly. Until this point, annual diagnosis is recommended for those who have relatives with retinal detachment or high myopia, that is, there is a predisposition to detachment.
If there is a predisposition to retinal detachment, at what age can it appear?
If there is a high degree of myopia, from -8, then it is quite early, even at 12-14 years old. There are people with congenital pathologies. But most often, thinning and rupture still coincide with physiological age, when the vitreous body begins to stratify, i.e. after 40 years. The vitreous gel begins to shrink and peel away from its attachment to the retina, creating tension and causing tears in the retina.
See a doctor immediately!
How is retinal detachment diagnosed?
Only an ophthalmologist can determine retinal detachment. One of the most important methods for diagnosing retinal detachment is the following:
In the photo (top left, clockwise) are examples of diagnosing retinal detachment: computer perimetry, tonometry, electrophysiological study (EPI), ophthalmoscopy
- Determination of visual acuity - to determine the center of the retina.
- Using computer perimetry, we examine visual fields and determine peripheral vision.
- We perform tonometry - we measure the patient's intraocular pressure.
- Electrophysiological study - to determine the viability of retinal and optic nerve cells.
- Direct and indirect ophthalmoscopy - an ophthalmologist examines the fundus of the eye, which allows you to determine the location of the ruptures, their number, and detect thinned areas in order to avoid further retinal ruptures.
After carrying out all diagnostic methods, the ophthalmologist can make a diagnosis.
Diagnosis of the disease
Identifying dystrophy and making a correct diagnosis involves conducting the following studies:
- Checking visual acuity (visometry).
- Identification of the visual field (perimetry).
- Check for distortion of visible lines - Amsler test.
- Detection of abnormal deviations in the refraction of light rays (refractometry).
- Biomicroscopy.
- Ophthalmoscopy.
- Determination of the degree of color perception.
- Electroretinography.
- Determination of the degree of adaptation of visual functions in the dark (adaptometry).
- Finding affected areas.
- Retino- and coherent tomography.
- Ultrasonography.
- Collection of analyses.
Depending on the clinical picture, the patient is prescribed a consultation with doctors of other specialties.
Operative methods
For rhegmatogenous retinal detachment, the following methods are used:
- Extrascleral. These include ballooning and filling.
- Endovitreal - vitrectomy.
- Cryocoagulation of ruptures.
- Laser treatment.
Extrascleral methods are effective only if the rupture, which resulted in a detachment, occurred recently (up to 1 month).
Ballooning is an operation that is performed on the surface of the tunica albuginea (sclera). The essence of the method is as follows: the surgeon identifies the location of the rupture and, accordingly, the detachment. After this, he sews a balloon made of elastic material to the tunica albuginea. This small container is then filled with gas or liquid. Gradually, an indentation area forms on the eyeball. Thanks to this, the membranes come together, resulting in the elimination of rhegmatogenous detachment. The operation is effective if no more than 1 of the 4 quadrants of the retina is affected.
Filling is a type of surgical intervention that is also performed on the surface of the tunica albuginea. At the diagnostic stage, the doctor determines the location, shape and size of the exfoliated area. Based on this information, a filling is made, consisting of a biocompatible material. As a rule, sponge silicone is used in ophthalmology clinics.
In case of retinal detachment, the operation is performed as follows: the surgeon makes an incision in the conjunctiva, through which a seal is applied to the site of the tear. After this, it is fixed with sutures. If the pathology is accompanied by severe swelling, drainage is performed. The final stage is suturing the conjunctival incision.
Vitrectomy is a surgical procedure during which the vitreous body is partially or completely removed. Instead, a substance with similar properties is introduced. This method is considered minimally invasive, since a minimum of perforations are made during the operation.
Cryocoagulation of fractures involves the use of low temperatures. The operation algorithm is as follows: the doctor drops an anesthetic drug into the patient’s eyes, while it begins to act, the surgeon lowers the cryoapplicator into liquid nitrogen. The latter is then placed on the eyeball. Through the use of ultra-low temperatures, a high penetration rate is achieved, while there is no effect on the tunica albuginea and muscle tissue. Cryocoagulation can be considered both as an independent and as an auxiliary method of treating rhegmatogenous detachment.
Laser treatment is also carried out under local anesthesia. This is a modern method, which is considered the safest due to the minimal risk of complications. In case of retinal detachment, the operation is carried out according to the following algorithm: the doctor directs a high-precision laser beam to the lesion, which promotes the fusion of the vascular and nerve membranes. The doctor monitors the progress of the operation using a microscope. Its duration is about 20 minutes, after it the patient can immediately begin his daily activities.
Treatment
The only treatment option is surgery. The choice of method will depend on the location of the defect, its complexity, and size.
There are several types of operations:
- sclerotherapy (the damage is sealed using diathermy (laser or current)). The tissue that is located around the retina becomes scarred and does not allow fluid to penetrate under the retina;
- pneumatic retinopexy (the defect is sclerosed using freezing or using a laser). Next, air is introduced into the eye into the vitreous cavity, which puts the retina in place;
- vitrectomy (two small holes are made in the sclera in order to have proper illumination of the surgical field, and a cutting emitter and thin tweezers are inserted inside). The removed vitreous is replaced by gas. After time, the gas dissolves and is filled with its own moisture;
- local filling (a small silicone filling is sewn onto the sclera, so that the sclera is pulled inward and together with the choroid, and comes closer to the retina);
- retinal ballooning (the essence of the method: a catheter with a balloon is temporarily sutured into the sclera in the area of detachment projection). The balloon is inflated and the same effect is obtained as when filling the sclera.
Treatment of retinal dystrophy
The standard treatment regimen for dystrophy using medication looks like this:
- Drugs that strengthen and dilate blood vessels. The dosage of Complamin, Noshpa, Papaverine or Ascorutin is selected individually for each patient.
- Medicines to prevent blood clots. This may be Aspirin, Ticlodipine or Clopidogrel.
- Vitamin B, administered intramuscularly, and a complex of other vitamins in tablet form.
- Medicines that prevent the formation of new painful blood vessels (Lucentis).
- Cholesterol-lowering drugs.
- Means for improving metabolism inside the eye. Injected intravenously or directly into the structure of the visual organs.
- Retinalamin, injected into the lower eyelid or eye shell for 10 days.
- Eye drops that speed up the healing process and metabolism.
Conservative treatment is complemented by physiotherapy. The patient is prescribed procedures such as photo- and electrical stimulation, electrophoresis, and magnetic therapy. If we talk about the use of small doses of laser radiation, they are used to influence the retina and blood.
Laser treatment
The laser beam extends its effect directly to the affected areas of the visual organs. They are exposed to irradiation in order to stimulate and start the metabolic process. The laser is able to strengthen blood vessels through their coagulation and separate affected areas from healthy ones, thereby stopping the spread of the disease. This process involves soldering defective tissues.
Surgery
If conservative and laser treatment methods do not help to cope with retinal dystrophy, the doctor decides to prescribe surgery. Depending on the complexity of each case, the following surgical interventions are performed:
- Revascularization – restoration of blood vessels.
- Vasoconstruction is a narrowing of the spaces between blood vessels.
- Vitretomy is complete or partial removal of the vitreous.
After surgery, it is necessary to take measures to help quickly restore visual functions. You need to make sure that your eyes are not overstrained, wear sunglasses outside, and take vitamins. In addition, it is necessary to stop smoking and excessive alcohol consumption.
Traditional methods of treating retinal dystrophy
Traditional medicine recipes for dystrophy should be used in conjunction with the main treatment regimen prescribed by the doctor. The following remedies have a good effect:
- Goat milk diluted with boiled water in equal proportions. Within a week, the resulting solution is dripped into the eyes, then covering them with a dark cloth. As a result, the process of retinal detachment will stop.
- For a month, drink half a liter of decoction per day. To prepare it, take 5 parts of pine needles, 2 parts of rose hips and onion peels. They are poured with boiling water and cooked for 10 minutes.
- A decoction of cumin and cornflower flowers is instilled into the eyes 2 times a day.
- For a month, a decoction of celandine is instilled into the eyes 3 times a day.
- Tinctures of birch, horsetail, lingonberry, and mustard are taken orally.
- Wheat grains are left to germinate in a warm place. The embryos grind and eat the resulting mixture.
- For 9 days, a decoction of mumiyo and aloe juice, boiled in proportions of 5:1, is dripped into the eyes.
Before using folk remedies, you need to consult a doctor and make sure that the components of the decoctions do not cause allergic reactions.
Please note: If, when a disease is detected, you refuse the help of a doctor and self-medicate, the disease may develop to a severe stage. It can lead to complete loss of vision, which is characterized by the irreversibility of the process.
Types of operations
In ophthalmology, there are several types of surgical interventions aimed at eliminating retinal detachment. Conservative therapy and traditional medicine do not provide a 100% guarantee of success. Therefore, when diagnosing pathology, it is recommended to immediately perform surgery.
Laser coagulation
The procedure is prescribed not only for retinal detachment, but also for thrombosis of the main vein, retinopathy, etc. The damaged area is cauterized with a laser beam, the operation takes a maximum of twenty minutes and does not cause pain in the patient. The doctor performs all procedures under local anesthesia, so coagulation is allowed even for elderly people and pregnant women.
The procedure causes virtually no unpleasant consequences. An anesthetic drug is instilled into the patient and his head is fixed. The laser beam is directed to a specific point and the fragments of the peeled shell are soldered together.
The main advantage of the method is the absence of pain and discomfort during the operation. Recovery takes a maximum of fourteen days. During regeneration, you must adhere to some restrictions: minimize eye strain, drive a car, and wear safety glasses before going outside.
Coagulation almost never causes complications; in exceptional cases, cataracts develop, swelling of the cornea or increased intraocular pressure is observed. The procedure is not recommended for opacification of the vitreous body and proliferation of the vascular system of the iris.
| To minimize the risk of developing negative consequences, follow medical recommendations and regularly visit your ophthalmologist. |
Extrascleral filling
The essence of the procedure is to apply an elastic silicone filling to the affected eye. It is soft, so it does not injure the eyes. It is fixed in the area of the rupture and secured with sutures. In this way, a protective barrier is formed that prevents further separation, and accumulated intraocular moisture is removed.
During the operation, an incision is made in the conjunctiva, and a seal is applied to the damaged area of the membrane. The fluid is removed using drainage instruments. Vision after extrascleral filling is restored gradually over six months. It is impossible to completely “reanimate” eye sharpness using the procedure.
Possible complications include infection in the wound, exposure of the installed filling, cataracts and increased pressure inside the eyes.
During the rehabilitation period, you should not lift weights or play sports, all of which can lead to the sutures coming apart. Be careful not to allow water or dirt to enter the operated eye. Be sure to use a protective bandage. Drops prescribed by your doctor will help minimize the risk of wound infection.
Vitrectomy
The essence of the operation is to remove the damaged vitreous and replace it with gas, silicone and other material. The procedure presses the retina against the sclera, helping to restore visual acuity.
During a vitrectomy, a microscopic incision is made through which instruments are inserted and the vitreous is removed. The operation lasts almost an hour and a half, there is virtually no pain due to the use of local anesthesia.
During the recovery period, minimize the load on the visual system, exclude sports exercises and temporarily stop using cosmetics. Renew the protective dressing periodically to minimize the risk of wound infection or inflammation activation.
| Among the negative consequences of vitrectomy, increased pressure inside the eyes and hemarthrosis are noted. The operation is prohibited if you have an allergic reaction or problems with blood clotting. |
Ballooning of the sclera
Treatment is carried out using a catheter with a balloon. Indentation of the sclera occurs due to the injection of fluid into the visual apparatus. The procedure is considered the least traumatic, but is used in exceptional cases.
Ballooning takes approximately fifty minutes. If you consult a doctor at an early stage of the disease, you can completely restore your vision. In the postoperative period, swelling and limited mobility of the eyeball are observed. On the first day after ballooning, it is necessary to maintain bed rest and minimize physical activity.
After surgery, complications such as cataracts and increased pressure inside the visual apparatus may occur. If there is hemorrhage or a large area of retinal tear, the procedure is not performed. Return to contents
What causes farsightedness in children
Children's farsightedness, along with strabismus and amblyopia, is one of the most common vision disorders. Children are born farsighted, but this problem usually corrects over time.
How is hypermetropia treated in children, does it create any restrictions?
Characteristics of farsightedness
According to ICD-10, each disease and disorder has its own code. Hyperopia – code according to the international classification system ICD-10 – H52.0.
Farsightedness - what is it? First of all, it is important to know that hypermetropia is not a disease. This is a disorder characterized by changes in the shape and size of the eyeball. The most common is axial childhood farsightedness, which is characterized by a deviation in the anteroposterior axis of the eye. We can say that farsighted visual organs are considered as not fully developed and are characterized by a delay in their growth.
At birth, almost every person is equally farsighted, and as the entire body grows, the sagittal length of the organ of vision increases. In newborns, the average eye length is about 18 mm, at two or three years old it is already 23 mm. From 4 years to 14 years of age, a child's growth slows down by about 0.1 mm per year. The length of the eyeball in older age is about 24 mm, which does not apply to hypermetropia of both eyes - in this case the length is shorter. The deviation value determines the degree of disorder. Degrees in children and adults are classified as follows:
- low degree hyperopia (plus 2 diopters, +2D);
- moderate hyperopia (plus 5 diopters, +5D);
- high degree hypermetropia (plus 5 diopters and above).
The treatment of farsightedness in children and the choice of correction method depend on the degree of the disorder (the first degree, as a rule, does not require correction; special exercises are used).
The shortening of the anteroposterior axis of the eye rarely exceeds 2 mm. A decrease in length of one millimeter represents a change in refraction of about plus 3 diopters.
Important! Improvement in vision (in most cases) during childhood distinguishes hyperopia in children from age-related farsightedness, called presbyopia.
Farsighted newborns and vision development
Natural farsightedness in children is associated with the shape of the eyeball. Newborns have imperfect vision at birth. Their eyes are immature and they do not perceive the outside world clearly. Therefore, there is no point in talking to them at a distance greater than 25 cm - they will see you blurry. Gradually, slowly, the baby builds eye contact with the people around him. Soon he can look at the offered toy, and at about 2 months he will begin to follow it with his eyes. Sometimes it happens that one eye squints, but for 6 months there is no need to worry - during this time, children's eyes develop, the interaction of both eyes and the visual centers in the brain. Thus, farsightedness in children under one year of age does not require correction. If a one-year-old child continues to have some degree of impairment, some restrictions on eye strain are needed. Doctor E.O warns about this. Komarovsky, who also recommends spending time with your baby outside more often - this will help speed up the improvement of vision.
At the age of six, a small person can see as well as an adult. Before this time, however, errors may occur that can disrupt the normal development of vision. During their stay in the maternity hospital, newborns are screened for cataracts as part of a general examination. The critical period for visual development is the first year of life, when binocular vision begins to form.
As mentioned, congenital farsightedness in children is normal. In only about 6% of young patients, hypermetropia values remain elevated, which can lead to strabismus and amblyopia in later life. These disorders are usually diagnosed before age 8. Vision development is completed during puberty, around 15 years of age.
Development of the disorder
In the case of farsightedness in children, the eye is unable to focus vision at close range. In general, this disorder manifests itself in such a way that a person has no problems contemplating distant objects, but cannot focus his vision on close objects. Farsighted people may have problems with reading and writing, cutting, gluing...
Farsightedness in children 1 year of age is most often caused by congenital shortness of the anteroposterior axis of the eyeball. Light rays are refracted behind the retina, not on it.
Important! Since the eyes are able to partially compensate for this problem by increasing accommodation, farsightedness may not be obvious in children under 3 years of age.
The disorder causes increased fatigue and headaches from excessive accommodation. Defective vision, like any ophthalmological disorder, can cause slow psychomotor development. Therefore, parents with farsighted children should consult an ophthalmologist. If necessary, the attending physician will prescribe a correction.
What causes hypermetropia
Genetic predisposition is responsible for many cases of refractive disorders, which include hypermetropia. But people also suffer from farsightedness of any degree, without having a genetic predisposition to this disorder.
In addition, environmental factors play a certain role in the development of farsightedness and its degree. However, heredity remains the best known cause, especially for the higher forms of this disorder (as well as other ophthalmic diseases).
The following factors involved in the formation of farsightedness are:
- flat cornea;
- insufficient refractive value;
- small lens thickness;
- congenital small visual organ (microphthalmos);
- short length of the sagittal axis of the eye;
- exposure to certain medications;
- injuries.
Farsightedness can also be caused by certain diseases (cancer, retinal detachment, etc.). In older people, provoking factors are decreased lens refraction and diabetes. Backward displacement of the lens due to illness or injury, aphakia (lack of an intraocular lens - lens) can also cause hypermetropia.
How to determine farsightedness in a baby
All parents should be attentive, especially in families where there is a history of visual impairment. There is a high probability of inheriting an ophthalmic disorder. Many parents, however, focus on the disorder when children start school, and problems with schoolwork may arise.
Farsightedness in a 2 year old child can be expressed as follows:
- while playing, he brings objects closer to his eyes, changes the viewing distance;
- when drawing, tilts his head over the table;
- the baby has an unnatural head tilt - in this way he can compensate for strabismus;
- periodically closes one eye;
- farsighted children quickly get tired when performing activities at close distances;
- they do not focus on details (pictures, toys);
- sit as close to the TV as possible;
- mistakenly determine the location of objects.
Important! If in any doubt, consult your pediatrician or ophthalmologist. He will assess the presence and extent of the disorder at an early age, and recommend opportunities for improvement.
How to help your baby
Below are some tips that you can follow to help maintain your eye health and vision.
- Daily Exposure to Natural Daylight – Scientific research indicates that everyone should spend at least 30-60 minutes a day outdoors in natural daylight. This rule does not mean direct exposure to sunlight!
- Limit watching TV and playing on the computer. They are sources of artificial light, which directly affects the quality of impaired vision. The maximum period for TV/computer is 30 minutes/day in total.
- Include physical activity in your daily routine. The type of activity does not matter - oxygenation of the body is important, preferably in the open air.
- If your child already wears glasses for farsightedness, let him take them off whenever possible.
- Provide a balanced diet rich in vitamins and minerals. Include as many fresh fruits and vegetables as possible (especially leafy green vegetables - spinach, cabbage, lettuce, etc.). Avoid white sugar (sweets, carbonated drinks) - it can be replaced with cane sugar. Make sure you stay hydrated.
Contact lenses and glasses
At what age can you wear contact lenses? Age is not a limiting factor in the use of contact lenses, it is a personal matter, depending on the particular child, his motivation, responsibility and ability to use contact lenses. Treatment of farsightedness in young children involves wearing glasses; children in the older age group can use lenses.
Lenses are usually worn throughout the day. The mode of wearing glasses is determined by the doctor depending on the specific condition. Usually, with low degrees of farsightedness, you can wear glasses only at school; in cases of moderate or severe impairment, you may have to wear them constantly. An important role is played by the presence of associated strabismus, amblyopia or astigmatism - for these disorders, correction is mainly permanent.
Prevention of retinal dystrophy
In order to reduce the risk of developing retinal dystrophy, you must follow these rules:
- Make sure your work area is properly lit.
- Any load on the visual organs should be accompanied by periodic rest.
- It is necessary to visit an ophthalmologist once a year.
- The diet should consist of foods containing vitamins and microelements necessary for normal metabolism.
- You need to give up bad habits (alcohol, smoking).
Massage and exercises strengthen the visual organs and normalize blood flow to them. Watch your health. Contact your doctor at the first signs of the disease to begin treatment on time.
Development mechanism
Rhegmatogenous retinal detachment is a multifactorial disease. This is a primary pathology resulting from rupture of nervous tissue.
There are two main mechanisms for the development of the disease:
- The occurrence of rhegmatogenous retinal detachment against the background of thinning of this layer. As a rule, this condition appears during the natural aging process of the body. For many people, the disease does not manifest itself in any way, but at the same time it can pose a health hazard. Over time, end-to-end defects form on the retina, through which fluid from the vitreous body begins to penetrate under it, causing detachment. In addition, often zones of dystrophy appear after injury to the eye.
- The occurrence of rhegmatogenous retinal detachment due to tension. The vitreous body is a gel-like substance that is 99% water. It is very tightly connected to the retina at the base of the latter, most weakly in the areas of localization of large blood vessels. During the natural aging process of the body, the vitreous body liquefies and the retina stretches. As a result, detachment occurs, which is not always accompanied by tissue rupture.
Since the disease is multifactorial in nature, in most cases both mechanisms are detected in patients at once. The risk of rhegmatogenous eye detachment increases significantly under the influence of provoking factors.
Possible complications and consequences
Retinal surgery is a rather dangerous procedure. Immediately after the procedure, the patient may experience ailments and extremely unpleasant sensations.
To get rid of them as quickly as possible, it is recommended to strictly follow the recommendations for the recovery period. If you ignore them, there is a high probability of negative consequences.
Among them:
- Inflammatory process. Typically, this condition manifests itself in the form of severe redness of the eyes, watery eyes and itching. To prevent such consequences, it is recommended to regularly drip your eyes with an antiseptic. It is best to continue this for 2 weeks.
- Decreased visual acuity. In the first few days, you may notice that your vision is blurry and it is extremely difficult to determine the outlines of objects. For 2-3 months you will have to wear glasses with different diopters. In addition, you should regularly visit your doctor throughout the year for detailed diagnostics.
- Strabismus. One of the most common complications of retinal detachment. Statistics show that a similar problem occurs in half of people who have undergone corneal surgery. Most often, strabismus occurs due to damage to the muscles of the eye.
- Increased intraocular pressure. A condition that, if not fully corrected, can lead to the development of glaucoma. To get rid of this problem, the patient needs repeated surgery.
- Repeated detachment. The probability of such an outcome is 25%. Most often, this condition can be treated with repeated surgery.
- Hemorrhage. This condition occurs due to mistakes made by the doctor during surgery.
- Narrowing of visual fields. Most often this occurs against the background of incorrectly selected power for laser coagulation.
Possible complications
Without timely intervention in angiopathy, a reversible change in the retina, tissue hypoxia and hemorrhage can be expected. The retinal vessels themselves also undergo changes. In turn, they become severely deformed and lose blood conductivity. In some cases, complete loss of vision is possible.
Complications can be caused by various bad habits, high blood pressure, hereditary vascular diseases, obesity, and high cholesterol.
Risk factors
Risk factors include both external and internal causes. There is a high probability of ruptures in persons diagnosed with myopia, when an enlarged eyeball causes thinning and rupture of the membrane. In old age, pathology is provoked by structural dystrophic changes in the vitreous body, leading to overstretching of the retina.
Pathological changes in the fundus, straining during childbirth, hypertension, diabetes mellitus and vascular diseases increase the risk of OS. All of them are associated with excessive tension and thinning of the retina. Serious ruptures are observed under the influence of traumatic factors and surgical interventions. During inflammatory processes, excess fluid accumulates in the subretinal zone, putting pressure on the retinal layer.
IMPORTANT! Every fifth child born prematurely suffers from retinopathy. In premature babies, the underdeveloped retina tends to rupture.
Contraindications for surgical measures for retinal detachment
Each type of surgical intervention has a number of limitations. For example, vitrectomy is prohibited in the following cases:
- With severe changes in the retina and cornea. In this situation, the operation will not bring the desired result;
- Significant clouding of the cornea. The pathology can be seen with the naked eye; it is presented in the form of an eyesore.
Filling has the following contraindications:
- Vitreous opacity;
- When the sclera protrudes.
Laser coagulation is not recommended for:
- Fundus hemarthrosis;
- Opacity of the organ of vision;
- Extensive retinal detachment;
- Anomalies of the vascular system of the iris.
| Also, do not forget about the restrictions in case of individual intolerance to anesthesia or the presence of an allergic reaction to an anesthetic substance. |
Surgery should not be performed if severe inflammatory processes are detected. For this reason, before prescribing the procedure, the doctor sends the patient for a number of additional examinations. It is necessary to pass all tests, undergo fluorography and get rid of caries. Return to contents